

At the time of this writing, it is December 31, 2015, and I am en route back to London after a holiday in Tanzania, where I was visiting my parents. With corneal tissue more easily available at Christmas time, I used the opportunity to do my usual stint of performing as many corneal grafts as possible just before Christmas at the CCBRT hospital in Dar-es-Salaam. Tissue was kindly donated by VisionShare (based in Michigan). As many of you who have worked in developing country environments know, a major recalibration has to take place in terms of priorities. With only eight corneas available and 25 patients listed for a graft, making choices was not easy. I rightly performed surgery on those who were bilaterally blind and in particular young patients. It was very gratifying to see the joy on the faces of those who benefited and heartbreaking for those disappointed by not being able to receive care.
Like many of you, I have spent the past few days reflecting on the year that has gone by. What went right? What did not go so right? In this process, I could not help but recall my journey in ophthalmology, how I got to where I am now, and how fortunate and thankful I am that I chose a career in medicine and the subspecialty of ophthalmology.
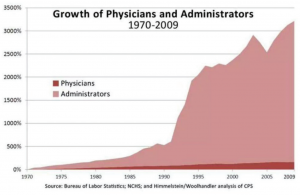
Figure 1. Growth of physicians and administrators in the United States and Canada.
Being a doctor is increasingly controversial these days. Recently, the UK junior doctors almost went on strike, and they are still likely to do so if talks fail. Other major issues include the increasing regulation and incredible bureaucracy in medicine that require greater and greater numbers of administrators. Figure 1 shows a striking graph reflecting the rise in administrators versus doctors from 1970 to 2009: a 3,200% increase versus 100% increase, respectively.
There are many reasons for the astonishing growth in administrators. Ostensibly, administrators assist medical activity, allowing doctors to spend more time doctoring. But this does not account for such a huge increase. Numbers have had to rise to accommodate increased regulatory activity and to deal with insurance companies, finance, and reimbursement. Numerous layers are created, with managers requiring minions to establish checks and balances of checks and balances. What an unbelievable waste, ultimately paid for by the patient either by way of increased insurance premiums, taxes, or self-pay fees.
Besides the problem of waste, the disproportionate number of administrators winds up controlling the medical establishment, as many readers I am sure will agree. There is an expectation for doctors to follow managerial processes that take considerable time away from patients, which often breeds resentment. I myself am a victim of this syndrome of management madness. Although I enjoyed working in the public National Health System (NHS) and directed my department with considerable growth on many fronts, I left after 17 years when, for the first time in my position, I started to be micromanaged, with constant harassment over trivialities ultimately leading to differences with the chief executive. I miss certain aspects of the NHS, including the challenging patients and camaraderie with colleagues and fellows; however, I am happy with where I am now in the private sector, leading my own show.
It is truly a pity that administrators underestimate the value of experienced doctors. A study by Goodall revealed that hospitals that had doctor-leaders were statistically significantly better in terms of quality outcomes than those led by non-doctors.1 The same author found in reviewing previous studies that expert subspecialists who were successful in their particular areas became better leaders in that area. Goodall also found that this applied to highly cited scholars, who made better presidents of universities.2 Additionally, the same author demonstrated that exceptional basketball players became better coaches3 and Formula 1 racing team leaders were better if they had previously been mechanics or drivers rather than engineers.4
In addition to having detailed knowledge of their field and its requirements, doctors understand other doctors, and, most important of all, they work in the interest of the patient—something that seems to have gone astray in many bloated health care systems and organizations. As professionals, doctor-leaders are likely to conduct themselves with integrity and work by example. Further, many aspects of being and behaving as a doctor are useful in management. Clinically, in dealing with patients, doctors must communicate well, often transcend to the level of the patient, and be able to negotiate with convincing, useful leadership skills. Surgeons often have to think many steps ahead and develop contingent alternatives. This is not too different from operational management, which is key to effective service delivery and efficiency. These are just a few of many examples of ways in which successful doctors make fine leaders.
An entire issue of CRST Europe would be required to cover this topic. In a nutshell, I would encourage colleagues to take leadership positions and take charge of their own futures. In ophthalmology, we are fortunate to be able to practice a great and rewarding specialty, and, unlike in many other specialties, we are truly able to create and lead organizations. For this, we must be thankful.
On behalf of my Co-Chief Medical Editor, Associate Chief Medical Editors, and the amazing staff at CRST Europe, I wish you a wonderful and successful 2016.
Sheraz M. Daya, MD, FACP, FACS, FRCS(Ed), FRCOphth
Chief Medical Editor
1. Goodall AH. Physician-leaders and hospital performance: is there an association? Soc Sci Med. 2011;73(4):535-539.
2. Goodall AH. Highly cited leaders and the performance of research universities. Research Policy. 2009;38:1079-1092.
3. Goodall AH, Kahn LM, Oswald AJ. Why do leaders matter? A study of expert knowledge in a superstar setting. J Econ Behavior Organization. 2011;77(3):265-284.
4.Goodall AH, Pogrebna G. Expert leaders in a fast-moving environment. IZA Working Paper No. 6715. July 2012.
