

Effective lens position (ELP) has been recognized as an important factor in IOL power prediction, and it is taken into account in many modern power calculation formulas. With no other IOL is ELP more important than with the Trulign Toric Accommodative IOL (Bausch + Lomb), and this is true not simply for purposes of predicting refractive outcome.
Despite a number of changes to the optic and haptics, the unique aspect of the Trulign (and of its parent platform, the Crystalens [Bausch + Lomb]), remains its hinged haptic design. But because of the toroidal posterior optic surface and the inherent induced astigmatic effect, even small degrees of IOL tilt or decentration can have a profound effect on refractive outcomes in the form of negative dysphotopsias,1 and, in severe cases, reduced BCVA.2
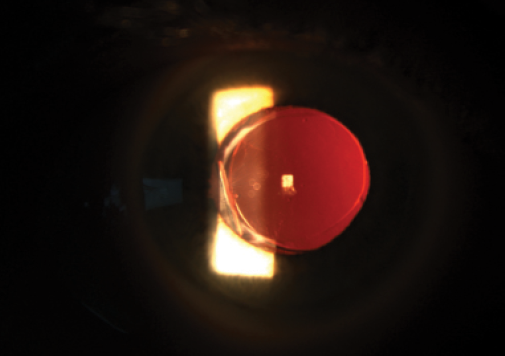
Figure 1. Trulign IOL with striae in the posterior capsule at the temporal hinge causing anterior displacement.
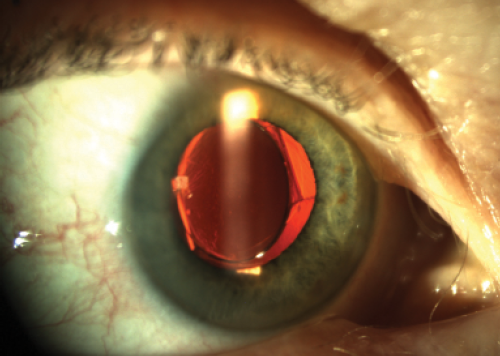
Figure 2. Trulign IOL with posterior displacement of the nasal hinge with evidence of significant tilt to the optic and induced on-axis astigmatism.
Tilting of the IOL, also known as the dreaded Z syndrome, is the result of uneven capsular fibrosis, in which contraction of the anterior, posterior, and even the equatorial capsular bag compresses the polyamide haptics disproportionately across the hinged plate-optic junction, forcing one pole of the optic anteriorly and the other posteriorly (Figures 1 to 4).3 Clinically, this results in a mild myopic shift in which the defocus equivalent increases as a result of significant astigmatism with the meridian orthogonal to the long axis of the lens. Fortunately, this is a rare complication.
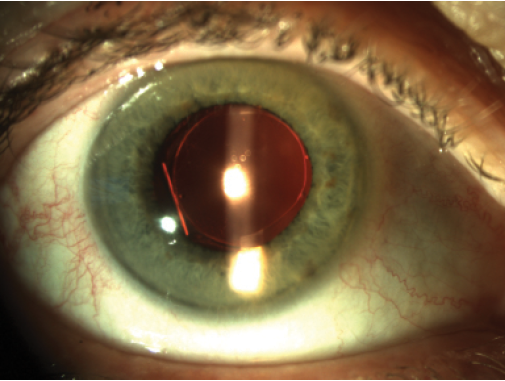
Figure 3. Transillumination axially shows 360° anterior capsular overlay.
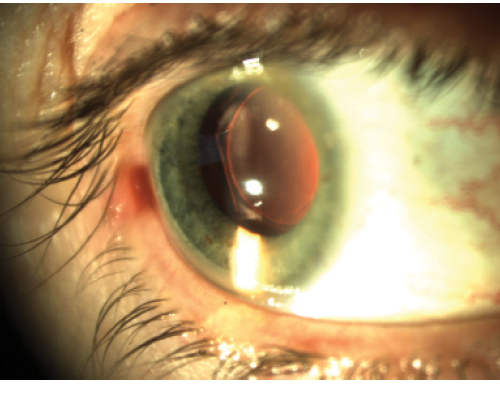
Figure 4. Trulign IOL with anterior displacement of the temporal hinge and posterior capsular contraction.
WHAT TO DO
A closer look at the etiology of Z syndrome provides the basis for its remediation. Management options to date are a source of debate, and, as with most arguments, there is no absolute right or wrong answer. In this article, I attempt to summarize the prevailing proposed solutions.2,4
The most obvious intervention, and the least invasive of the surgical options, is to perform Nd:YAG laser capsulotomy. Unlike the typical treatment of a fixed monofocal IOL, however, it is suggested that this be performed in a sequential manner over multiple visits, beginning with opening the posterior capsule behind the anteriorly displaced hinge. Should the lens tilt persist, an opening is created in the central capsule behind the optic, with care taken to avoid connecting the two rents. Finally, anterior capsular radial tears are placed to relieve the anterior capsular contraction.
The pattern of this anterior capsulotomy is another source of disagreement. The prevailing technique is to start at the short axis, perpendicular to the force of contraction on either side of the optic, in an effort to lay down as few radial spots necessary to release the traction band. Others have suggested placement of radial cuts at either side of the capsulotomy outside of the haptic-optic junction at the posteriorly displaced pole.
Alternatively, surgical manipulation of the Crystalens platform that is locked in a Z configuration has been suggested in cases in which the IOL is displaced to such an extent that there is clearance between the posterior capsule and the posterior surface of the optic or haptics. The belief is that laser capsulotomy will not sufficiently release the traction to effectively reduce the tilt because the haptics are likely not sitting in the equator of the capsular bag. In this maneuver, once the lens optic is rotated free of endocapsular adhesions, when possible, the IOL is rotated 90°, and a capsular tension ring (CTR) is placed.
I have met with success and failure with both laser and surgical options. To be more specific, I have been in the situation where initial surgical management failed to completely release the posterior capsular contraction following CTR placement, and fixed posterior striae were present despite careful dissection of the haptics from their peripheral endocapsular position and free rotation of the IOL. As a result, the IOL remained asymmetrically compressed until YAG capsulotomy was performed 6 weeks later. Conversely, I have had to explant the Crystalens when it was fixed in a Z configuration despite aggressive YAG capsulotomy.
It is safe to say that the best way to achieve optimal results with the Trulign/Crystalens platform is to handle with care. In other words, the image quality and enhanced range of vision that are achieved with the accommodative platform are worth a little extra attention, and this complication is not so insurmountable as to warrant depriving patients of the increased spectacle freedom that can be achieved when the lens is implanted and functioning correctly.
PATIENT SELECTION
I follow a few simple rules when it comes to selecting patients for implantation of the Trulign or Crystalens. Sometimes, patients express a desire for placement of the Crystalens or Trulign after researching the technology, and in other situations I raise the possibility of addressing presbyopia at the time of crystalline lens removal. Either way, initially there are a few things I consider as part of every evaluation.
AT A GLANCE
• Because of their hinged haptic design, the Trulign and Crystalens (Bausch + Lomb) remain subject to the possibility of Z syndrome.
• Patient selection and surgical technique are both important in avoiding Z syndrome.
• Several recent updates to surgical technique and instrumentation have provided excellent results with this lens platform.
I do not place the Trulign or Crystalens in eyes with an axial length shorter than 22 mm or with pseudoexfoliation syndrome or evidence of zonulopathy. When the axial length is greater than 25 mm, I routinely place a CTR to ensure that the longer platform is seated appropriately.
Furthermore, a central capsulorrhexis of uniform shape and size (5.5 mm) is imperative. Fortunately, the bi-aspheric optic design can account for a visual system with mild angle kappa. With this in mind, I temporarily gravitated to the femtosecond laser for creation of the anterior capsulotomy when implanting the Trulign or Crystalens. This device generated well-centered, perfectly sized and shaped capsulotomies, and my early results were impressive. However, I encountered capsular contraction that I had not experienced previously, and this was consistent with others’ anecdotal reports of increasing frequency of Z syndrome with use of the femtosecond laser. The theory (anecdotal information from Crystalens Users Meeting) that has been proposed is that the laser energy at the capsulotomy edge combined with residual lens epithelial cells and accelerated fibrosis.
A FEW UPDATES
As a result of recent Z syndrome following femtosecond capsulotomy, I have returned to the basics, with a few updates. I have increasingly been using the LessDrops formulations (Imprimis Pharmaceuticals) for all of my refractive procedures. However, my Trulign or Crystalens patients are still treated with a daily steroid drop for more than 2 months after surgery, with the intent of achieving a very slow and controlled collapse of the capsule around the IOL.
I have also been able to achieve a femtosecond laser–like capsulorrhexis with use of the Verus capsulorrhexis device (Mile High Ophthalmics), and I often double down by using the Callisto Eye Cataract Suite (Carl Zeiss Meditec) to project the patient’s visual axis as measured by the IOLMaster 500 (Carl Zeiss Meditec). As a result, I can create a near-perfect 5.5-mm capsular opening without worrying about activating lens epithelial cells and inducing capsular phimosis.
When I place a fixed monofocal toric IOL, I often leave the undersurface of the anterior capsule unpolished to reduce the likelihood of lens rotation. With the Trulign or Crystalens, on the other hand, the four-point open-loop haptic design needs no assistance to achieve rotational stability. Therefore, I am free to fastidiously polish all visible capsular surfaces, which are presented with unbelievable contrast under the OPMI Lumera 700 microscope (Carl Zeiss Meditec).
Finally, with few exceptions, I perform Nd:YAG laser capsulotomy on all Trulign or Crystalens patients at the 3-month visit prophylactically to ensure adequate contraction at the equator of the capsular bag complex, with or without the assistance of a CTR.
CONCLUSION
I suspect that, as long as we continue to implant accommodative IOLs in the human eye, issues with regard to ELP and concerns over unwanted tilt and the possibility of Z syndrome will persist. However, when I am careful to adhere to the basic tenet that an ounce of prevention is worth a pound of cure, I find that my patients and I experience great success with the Trulign/Crystalens platform.
1. Ortega ARG, Higueras A, Ortiz-Gomariz A, Valverde AN, Villa-Collar C, Gonzalez-Meijome JM. Correction of negative dysphotopsia in Crystalens “Z Syndrome.” J Emmetropia. 2013;4:101-104.
2. Yuen LH, Lee SY, Chua WH. Severe Z syndrome with the plate-haptic silicone hinged accommodating IOL. Paper presented at: American Society of Cataract and Refractive Surgery Annual Meeting; April 9-14, 2010; Boston, MA.
3. Qi Y. Crystalens Toric IOL, Literature Review. Memorandum; Department of Health & Human Services: February 22, 2013. http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/OphthalmicDevicesPanel/UCM346412.pdf. Accessed December 18, 2015.
4. Harvey Carter. To Yag or Not to Yag [Video]. Sponsored by Bausch + Lomb. http://ophthalmologyweb.cnpg.com/Video/flatFiles/1849/index.aspx. Accessed December 19, 2015.
Jonathan D. Solomon, MD
• Surgical/Refractive Director of Solomon Eye Associates, Bowie, Maryland
• jdsolomon@hotmail.com
• Financial disclosure: Consultant (Bausch + Lomb, Carl Zeiss Meditec)
