

Over the past 5 years, the volume of LASIK procedures in young patients has either declined year after year or, at best, has remained flat. The availability of a presbyopic LASIK treatment, namely Supracor (Bausch + Lomb), has opened the door for us to attract a new market segment for laser refractive surgery. This development has enabled us to treat not only precataract presbyopes, aged 40 to 60 years, but also to increase our cataract volume. That is because patients who were not aware they had developing cataracts came for Supracor screening and, when they learned they were on the way to cataract surgery soon, opted to receive treatment with presbyopia-correcting IOLs.
Supracor is a propriety presbyopia algorithm that corrects refractive error and presbyopia in a one-step procedure using the Technolas 217P or Teneo 317 excimer lasers (both from Bausch + Lomb). The Supracor software creates a 12-µm elevation with negative spherical aberration in the central cornea surrounded by an aspheric-optimized midperipheral zone (Figure 1). The central hyperprolate area extends the eye’s depth of focus approximately equal to 2.00 D of near addition. As the patient accommodates and the pupil constricts, the eye sees more through the central near addition zone, whereas when the patient looks at a far object and the pupil dilates, the aspheric-optimized midperipheral zone improves distance vision.
CLINICAL EXPERIENCE
I have been offering Supracor treatments to hyperopic and myopic presbyopes for the past 3 years. We also participated in a clinical study of Supracor in pseudophakic and post-LASIK eyes. My strategy is to apply the Supracor treatment to the nondominant eye to aid in near vision and to perform standard LASIK for good distance vision in the dominant eye.
With 2-year follow-up, patients in our practice undergoing hyperopic Supracor LASIK treatments have achieved a mean manifest refraction spherical equivalent (MRSE) of -0.58 D, distance UCVA of 20/25, intermediate UCVA of 20/20, and near UCVA of J1. Those undergoing myopic Supracor treatments have achieved a mean MRSE of -0.75 D, distance UCVA of 20/40, intermediate UCVA of 20/25, and near UCVA of J1. Because the dominant eye is targeted for optimal distance vision, mean binocular UCVAs for both the hyperopic and myopic groups were 20/25 distance, 20/25 intermediate, and J2 near.
.png)
Figure 1. The Supracor procedure creates a 12-μm elevation with negative spherical aberration in the central cornea surrounded by an aspheric-optimized midperipheral zone.
AT A GLANCE
• The availability of a presbyopic LASIK treatment has opened the door for surgeons to attract a new market segment for laser refractive surgery.
•Patients are attracted to Supracor because it is a LASIK-based procedure.
• With a mini-monovision strategy, patients’ binocular UCVA is good for distance, intermediate, and near.
CAUTIONS
Patients are attracted to Supracor because it is a LASIK-based procedure. LASIK is familiar to them, and most likely one or more of their friends or relatives has experienced it. For an experienced LASIK surgeon, the procedure is straightforward with no learning curve. However, two points must be emphasized.
First, the refractive target for Supracor is not plano but rather -0.50 to -0.75 D, to further enhance the 2.00 D addition of the central near zone. This makes the near UCVA vision J2 to J1, but the distance UCVA stabilizes at approximately 20/30. BCVA remains 20/20. Patients’ expectations have to be managed because, although their near vision will be significantly improved, distance vision may not be as sharp as they expected it to be. I believe at least one eye should be corrected for very good distance vision, or else the patient will be unhappy. This is why I have avoided doing bilateral Supracor treatments and have persisted in using a mini-monovision strategy.
Second, proper centration for the Supracor procedure demands attention. My recommendation is to center the treatment on the corneal light reflex (Purkinje reflex) in order to ensure that the patient looks through the near add zone to maximize near vision.
The extended-depth-of-focus effect of Supracor is not without limitation or compromise. The more near vision we target, the more we sacrifice distance UCVA; however, we do not sacrifice as much as we would expect in classic monovision. Because mini-monovision is my recommended treatment plan, it is imperative to perform reliable dominance testing and ascertain which eye the patient will tolerate to be more blurry for distance.
Glare is not a common complaint, but patients may notice a mild halo effect at night that is reported to fade over 6 months. Because Supracor is a LASIK-based procedure, we have observed regression in some eyes to a magnitude of approximately 0.50 D over 2 to 3 years. In hyperopic presbyopes, from an initial myopic outcome, regression results in refraction shifting toward plano or mild hyperopia, improving far vision but reducing the near vision that was initially achieved. At the beginning of my experience with the procedure, I aimed for -0.50 D in hyperopic presbyopes, but now I use -0.75 D as my refractive target regardless of age, in order to delay regression. Myopes, on the other hand, tend to regress toward more myopia, so their near vision improves over time but distance vision suffers. I previously targeted -0.75 D in myopes, believing that any less myopia would cause dissatisfaction because patients are used to having good near vision to begin with. However, I now target -0.25 D to avoid sacrificing too much distance vision, and I expect the regression over 6 to 12 months to cause an improvement in near vision.
DEALING WITH DISSATISFACTION
It is unavoidable to have some unhappy patients. The reasons can include off-target refractive outcomes, insufficient Supracor effect at the outset, poor distance vision, regression either in refraction or vision, visual disturbances, and difficulty in adjusting to the monovision effect. Retreatments provide a remedial mechanism to reduce dissatisfaction. I categorize retreatments into three types:
- Type 1 is refractive enhancement, wherein I adjust the patient’s refractive outcome by using standard LASIK touchup protocols to get him or her to target refraction.
- Type 2 is Supracor enhancement, wherein I add another Supracor treatment over a previous Supracor.
- Type 3 is reversal, wherein we use wavefront-guided LASIK to reverse the Supracor effect. We are unable to use topography-guided LASIK software because it is not enabled on our excimer laser.
Table 1 shows our retreatment rates.
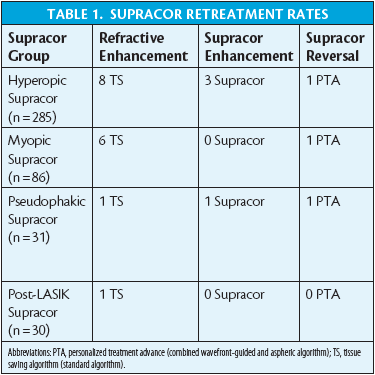
For patients who want to improve the near UCVA outcome of Supracor but whose distance-corrected near UCVA is J3 or better, we believe they have achieved some amount of Supracor effect, so we perform a refractive enhancement to achieve a refractive outcome of -0.75 D. If their distance-corrected near UCVA is worse than J3, that means they do not have a Supracor effect; therefore, adding another Supracor treatment with a target of -0.75 D is the recommended course of action. If patients are unhappy due to a significant decrease in distance vision, or if they experience double images and significant glare and haloes, they may opt to have their Supracor reversed.
We published a case report of Supracor reversal because of a decentered Supracor treatment that resulted in refractive error and significant glare and haloes. After reversal, the patient’s distance UCVA improved, and photic phenomena significantly decreased.1
CONTINUED LEARNING
After 3 years of experience with presbyopic LASIK, we continue to learn more about the algorithm and tighten the nomogram. Supracor is my top choice for presbyopia treatment because it can correct refractive error and presbyopia simultaneously in one procedure. Supracor benefits from the high degree of awareness and acceptance of LASIK. Patients experience significant improvement in near and intermediate UCVA but do not experience the huge anisometropia effect often seen in classic monovision. With a mini-monovision strategy, patients’ binocular UCVA is good for distance, intermediate, and near. Most important, we can adjust or reverse the Supracor effect, if necessary, to improve patient satisfaction.
1. Ang RE, Reyes RM, Solis ML. Reversal of a presbyopic LASIK treatment. Clin Ophthalmol. 2015;9:115-119.
Robert Edward Ang, MD
• Senior Consultant, Asian Eye Institute, Makati City, Philippines
• rtang@asianeyeinstitute.com
• Financial disclosure: Research Investigator, Consultant (Bausch + Lomb)
