
Getting to Know the Patient
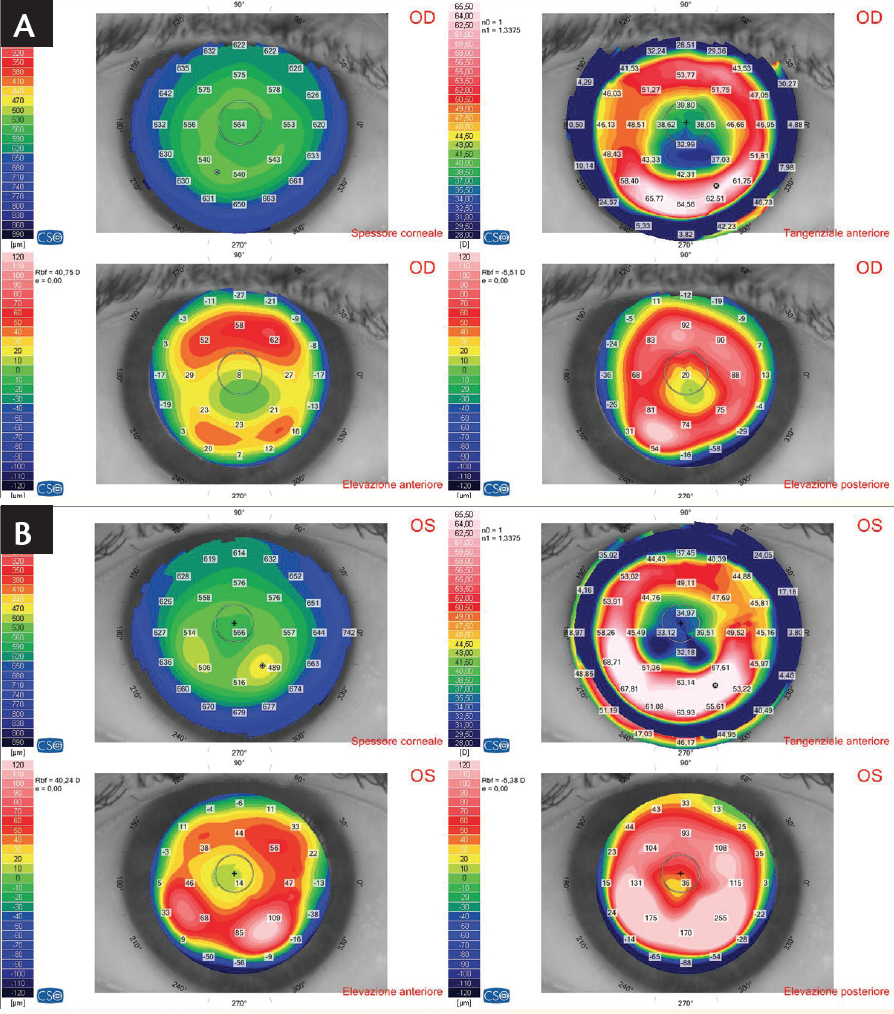
Figure 1. Corneal tomography in the patient’s right (A) and left (B) eyes showed a small central area of significant flattening.


In our experience, the central part of the cornea after RK is flatter than is measured either by automated refraction or by corneal topography.1,2 Therefore, we find it necessary to remeasure the post-RK patient’s visual acuity, looking for the maximum positive lenses. In the specific case described in Getting to Know the Patient, the results in the patient’s right and left eyes were 4.00 and 4.25 D sphere, respectively. With these lenses, the patient’s distance BCVA was the same as with his (lower) distance correction, and his near BCVA was the same as with his near vision correction.
With our examinations completed, we identified three preoperative concerns in this case:
- No. 1: Existing RK with incisions crossing the corneal limbus;
- No. 2: Multifocal corneas in both eyes; and
- No. 3: High astigmatism and coma in the right eye, apparently not disturbing the patient’s vision.
Given these concerns, what surgical approach would be best, and which IOL?
PREOPERATIVE PLANNING: THREE DECISIONS
When planning surgery in this case, we had to make three key decisions.
Decision No. 1: Not to employ laser-assisted cataract surgery (LACS). Although successful LACS after RK has been described in the literature,3-5 the fear of creating capsulotomy bridges prompted us to prefer microincision cataract surgery (MICS), a procedure that requires an incision of only 1.8 mm.6

Figure 2. The Incise IOL, an aberration-free spherical lens.
Decision No. 2: Choice of IOL. We decided to use a spherical IOL because the patient had always used spherical spectacle lenses with reported good distance BCVA before the cataract developed. We selected the Incise MICS IOL (Bausch + Lomb; Figure 2) for several reasons:
- The need to implant the IOL through a sub–2-mm incision, even considering the high dioptric power probably required;
- The aberration-free design of this IOL, which makes it perfect for use in eyes with compromised corneas;
- The subjective irrelevance of the corneal astigmatism, which allowed us to select a spherical IOL;
- The high Abbe number of this IOL, with good color vision results to be expected;
- The low rate of posterior capsular opacification we have experienced with this IOL; and
- The ease of explantation should either eye require IOL exchange.
The Incise IOL is made of a hydrophilic acrylic material with 22% hydration; it is rigid and has a good square posterior edge. This lens is popular in Italy in conjunction with MICS, as it can be implanted through a 1.6-mm incision with a wound-assisted technique or through a 1.8-mm incision with in-wound implantation through a 1.5-mm injector.7
Decision No. 3: IOL power calculation. We used the calculation sheets provided by the IOLMaster (Carl Zeiss Meditec) and by the American Society of Cataract and Refractive Surgery (ASCRS) online IOL calculator for eyes after refractive surgery (Table 1). After considering the patient’s multifocal cornea, the central corneal flattening within the circumference measured by the IOLMaster, and the preoperative refraction, we selected powers of 25.50 and 30.00 D for the patient’s right and left eyes, respectively, with the purpose of providing some pseudoaccommodation. If the IOL power proved to be too high, we would have the ability to exchange the IOLs if the patient could not tolerate the mild myopia; if it proved to be precisely right, the patient could be spectacle-free for a number of years.
SURGERY
Surgery in the patient’s left eye took place in August 2015 and was uneventful. We were able to place the 2-mm incision between two radial cuts without opening them (Figure 3) and to implant the lens without problems (Figure 4). After surgery, we immediately noted good distance and near UCVA (0.12 and 0.14 logMAR, respectively), even though the autorefractor now indicated a refraction of -2.00 -3.00 X 170°.
Figure 3. The corneal incision is placed between two of the RK cuts.

Figure 4. IOL implantation between two RK cuts was accomplished without opening the incisions.
Surgery in the second eye was performed using the planned IOL power, again with good postoperative distance and near UCVA (0.08 logMAR and 0.01 logMAR, with -1.75 D myopia measured by automated refraction, respectively).
CASE RECAP
WHO
61-year-old man with decreased vision, especially for distance, who had undergone 12-incision bilateral RKs in which the cuts crossed the limbus; he now presented with cortical cataracts, a small central area of significant corneal flattening, astigmatism, and a large degree of coma aberration that was not perceived by him
WHAT
Decide how to (1) plan surgery given that the existing RK incisions crossed the corneal limbus, leaving not much room for cataract surgery incisions, and (2) select an IOL to provide the patient with the best vision despite his compromised corneas
How
A MICS technique requiring an incision of only 1.8 mm and implantation of a spherical IOL that is compatible with MICS
The patient is now spectacle independent. His multifocal cornea provides the amount of pseudoaccommodation required for near vision: a further indication that corneal topography still must be backed up by clinical assessment, despite the precision of the machines now available.
LESSONS LEARNED
Careful planning, considering not only the objective technical data but also the patient’s history and subjective preferences, was an important basis for the success of surgery in this case. So too was the availability of an IOL with an aberration-free profile that is suitable for MICS implantation. We recommend use of the Incise IOL for any patient after RK or other forms of corneal refractive surgery.
1. Bellucci R, Palamara A. Automated refraction in eyes with radial keratotomy [in Italian]. Boll Oculist (Rome). 1994;73(Suppl 3):63-67.
2. Seitz B, Langenbucher A. Intraocular lens power calculation in eyes after corneal refractive surgery. J Refract Surg. 2000;16(3):349-361.
3. Whitman J. Victus femto laser capsulotomy in post RK cataract surgery. https://www.youtube.com/watch?v=muoFf0dvD2c. Accessed May 11, 2016.
4. Jones J. Catalys femtosecond laser cataract surgery. https://www.youtube.com/watch?v=qX4kLGq1HS4. Accessed May 11, 2016.
5. Wong S. LenSx laser cataract surgery technique 5-14-12. https://www.youtube.com/watch?v=jptn-bx8qQk. Accessed May 11, 2016.
6. Alió JL, Elkady B, Ortiz D. Corneal optical quality following sub 1.8 mm micro-incision cataract surgery vs. 2.2 mm mini-incision coaxial phacoemulsification. Middle East Afr J Ophthalmol. 2010;17(1):94-99.
7. von Sonnleithner C, Bergholz R, Gonnermann J, Klamann MK, Torun N, Bertelmann E. Clinical results and higher-order aberrations after 1.4-mm biaxial cataract surgery and implantation of a new aspheric intraocular lens. Ophthalmic Res. 2015;53(1):8-14.
Roberto Bellucci, MD
• Chief Ophthalmic Surgeon, Unità Locale Socio Sanitaria No. 20, Verona, Italy
• robbell@tin.it
• Financial disclosure: Consultant (Bausch + Lomb)
Angela Panico, MD
• Ophthalmic Surgeon, Unità Locale Socio Sanitaria No. 20, Verona, Italy
• angy.panico@gmail.com
• Financial interest: None acknowledged