



German ophthalmologists who own solo rural practices today have a hard time finding young colleagues who are willing to take over the practice when they retire. Their younger colleagues tend to want to work in large medical centers where their focus can be much more on clinical than on administrative work. Yet in my opinion, a surgeon-led practice is still the most ideal practice model, and herein I describe why.
FROM A SINGLE CENTER TO AN AMBULATORY HEALTH CARE CENTER
I have been working in my practice now for more than 25 years. When I started, our team consisted of three ophthalmologists and two residents, and the practice was located only in Ahaus, a medium-sized town of 40,000 inhabitants in Northwest Germany, 12 km from the Dutch border.
During the past 12 years, I have changed the organization of the practice to an ambulatory health care center rather than a group practice. This means that, apart from my business and professional partner, Olaf Cartsburg, MD (Figure 1), all our other colleagues are employed by the practice. We changed the name of the practice to Augen-Zentrum-Nordwest to illustrate its size and reach—thanks to the satellite practices that we have acquired throughout the years.

Figure 1. Stefanie Schmickler, MD (left); and Olaf Cartsburg, MD, are co-CEOs of Augen- Zentrum-Nordwest, in Ahaus, Germany.
Augen-Zentrum-Nordwest consists of a flagship practice located downtown in Ahaus, its large eye clinic located on the campus of our local hospital, and nine other practices in towns up to 80 km away (Figure 2). In the course of 1 year, we see more than 130,000 patients; perform more than 12,000 surgeries; and offer a wide range of consultations, treatments, and therapies. Our colleagues who refer patients to us also consider us a second-opinion center.
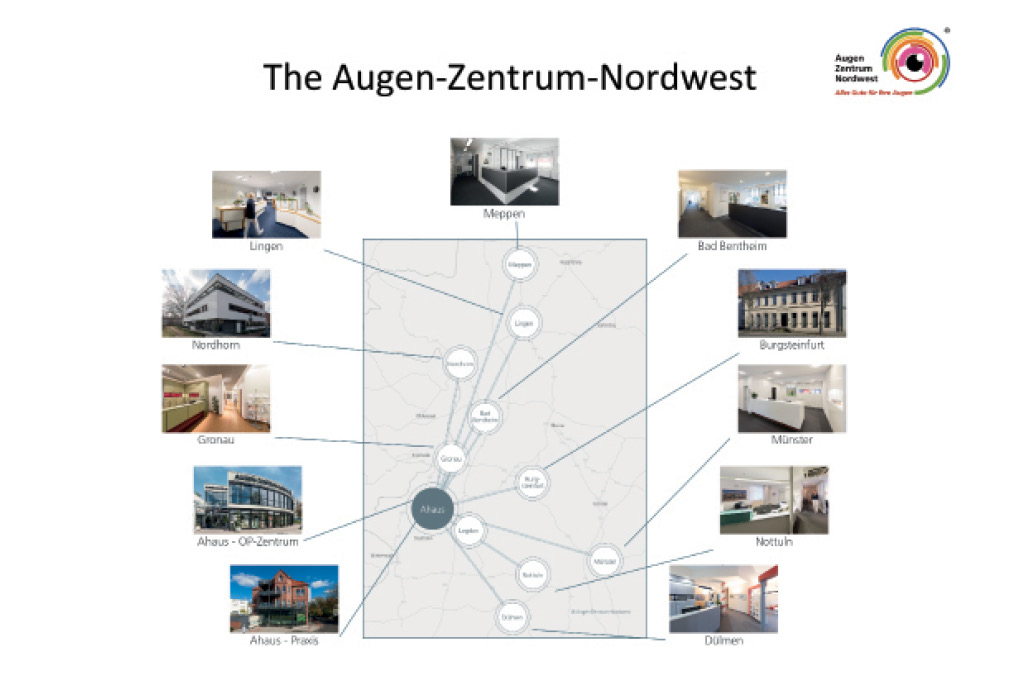
Figure 2. The flagship practice and the Ahaus eye clinic of Augen- Zentrum-Nordwest are linked with nine satellite practices.
Of course, we could be even more efficient if we only performed surgery. But, for all of our colleagues, the relationship we have with our patients is highly important. We can accompany patients from diagnosis through their therapy and even see them for follow-up over many years. Therefore, we gain great experience, for example knowing how IOLs look after years in the eye, in regard to glistenings, the incidence of posterior capsular opacification, and other variables.
A PASSION FOR THE PRACTICE
The medical market has recently become attractive for investors. I am not convinced of the value of the corporate practice concept. For me, the practice is my passion. Unlike with corporate practices, for me it is not just about maximizing profit but rather about maximizing patient happiness, which can only be achieved by a dedicated team.
I can also decide who should join my team and who I need to let go. In a state hospital, surgeons have to accept the dictates of the business administration—for example, which nurses are hired. I can confront my team members if something goes wrong and praise them if something goes right.
Furthermore, we have no predefined surgical quotas. We do not have a defined number of surgeries to be performed in a month or a year. Quotas can lead to soft indications, or unjustified surgeries. I could lose my reputation if I ran my practice driven purely by the number of surgeries performed.
EQUIPMENT DECISIONS
A further advantage of a surgeon-led practice is that we can make fast decisions, as we are not dependent on the rulings of a business department. I can decide what equipment we buy and base that decision on what we really need, not necessarily on return on investment. For example, CXL is a rather cost-ineffective procedure, but it is an important therapy that must be accessible to our patients.
About 2.5 years ago, we were unsatisfied with the femtosecond platform we used for laser cataract surgery, for which there was a per-procedure fee. We decided to give the laser back, and within 2 days we bought the Femto LDV Z8 (Ziemer Ophthalmic Systems). With the mobile unit, we save time during surgery because the patient does not have to be relocated from laser bed to operating table. And with this new approach to laser cataract surgery, we have increased our numbers of private patients. The new laser enables a more efficient workflow, and it incorporates up-to-date technology that also leads to greater satisfaction among the surgery team members.
Ziemer is a company with similar values to our own, interested in exchange of information between clinic and manufacturer. We learn from them, and, vice versa, they learn from our experience. We maintain a similar collaboration with Schwind eye-tech-solutions. We were users of their first excimer laser, the Esiris, and now we use the company’s Amaris 550. My business partner and I are able to negotiate with the leaders of these companies and affect the development of their products. In return, the companies appreciate our stability and reliability as customers.
Despite these relationships, if we are unhappy with a product we have been using, we eliminate it and look for a better solution. By doing this, we maintain a better commitment to our eye center and its patients.
PATIENT AND TEAM SATISFACTION
Every month, we generate a cost-performance analysis so that we can decide quickly if anything is going wrong within the practice. However, we always try to see the big picture and not be only price-driven. For example, we do strabismus surgery, which is not very cost-effective. However, we think of it this way: A child may need strabismus surgery now, and, if we do a good job, years later that child's grandmother will come to us for cataract surgery.
The key to success is to concentrate on patient satisfaction. In our surgeon-led practice, we feel deeply committed to our patients, some of whom we have served over years and even decades. But we also pay attention to our team’s satisfaction. We do a lot for our employees, including subsidizing child care and helping with parking charges or electric bikes for commuting. We are thankful for the dedication of our team, and we try to show it (Figure 3). We must be doing something right: Due to a high level of team satisfaction, we have less turnover than is seen in corporate practices.

Figure 3. The team made a trip to the German football museum in Dortmund, in combination with attending a conference on CXL.
With regard to marketing, we have the ability to promote our clinic and our special treatments according to our patients' needs, which we know well after 25 years of servicing them. Advertising rules vary across Europe, as do cultural differences. A corporate practice would have the same marketing concept across Germany and Europe, but we can address our own local audience as appropriate.
A MEANS TO HEALTHY GROWTH
In summary, our clinic is growing healthily because of our healthy internal systems. In this surgeon-led practice, I can concentrate on factors that improve my daily processes. I can analyze employee satisfaction and work with staff members to improve things if morale is low. I also can work with companies to maximize the performance of the products we use. And we can appeal to our local patient population with marketing that is appropriate to the region.
Our growth is dependent not only on the number of patients we see for surgery, but on the dedication of our physicians and staff to serving those patients in the best ways we can.
