



Ophthalmologists are all about vision preservation and vision restoration, and refractive surgeons add vision correction to that list. Optometrists are also in the business of improving the quality of vision, and hence the quality of life, for their patients. Our disciplines are therefore broadly aligned in our respective missions.
I find it difficult to understand the unhealthy competition that goes on between ophthalmologists and optometrists in some areas around the world. In some countries, it may even amount to blatant disregard. This is sad and unproductive in my view; both parties are committed to improving their patients’ vision and therefore share this goal. The way I see things, the burden of eye conditions that will affect our patients’ eyes in their later years is only increasing (see By the Numbers). It makes a lot more sense to work together to achieve common goals than to see each other as competitors and our services as mutually exclusive.
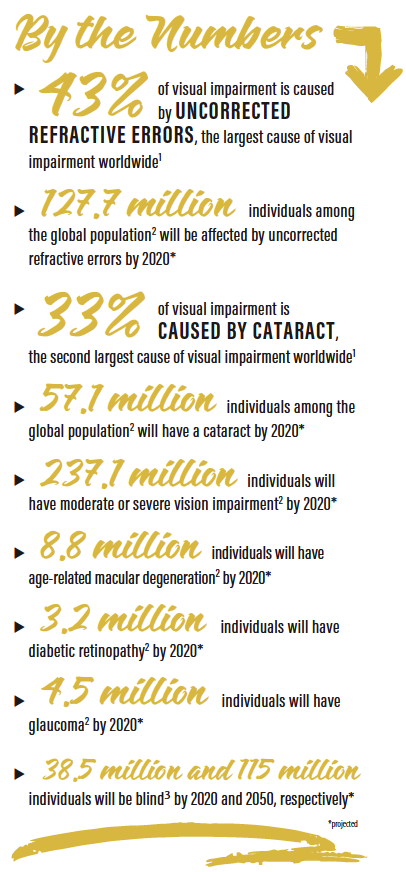
As the population ages, the incidence of cataract, glaucoma, age-related macular degeneration, and diabetic retinopathy and maculopathy are all destined to increase and to place ever-greater burdens on the shoulders of ophthalmologists and on the already overstretched public health care sector. Having the optometric community help share the burden of this workload is a win-win solution.
AREAS OF OVERLAP
The overlap between the two professions covers several subspecialist areas where comanagement may be a good solution.
Scenario No. 1. First, in a patient with a developing cataract, the optometrist notices the reduced vision and increased symptoms in the patient and the fact that spectacle correction is no longer providing adequate visual acuity. The patient is referred with cataracts and is ready for surgery having already discussed the risk:benefit ratio in broad terms with the optometrist. At the ophthalmologist’s office, then, it’s a matter of performing the biometry and OCT of the macula and scheduling surgery if the patient selects to proceed. The day 1 postoperative visit is managed by the ophthalmologist’s office, and the day 7 and the >week 4 to 6 visit> is performed by the comanaging optometrist.
Scenario No. 2. If the patient has a residual refractive error and wants to improve his or her vision, the optometrist either provides spectacles or refers the patient for refractive surgery. Here again, the optometrist will be involved on the front end as well as the back end of surgery, as the follow-up visits any time beyond day 1 are performed by the optometrist.
Scenario No. 3. In the event that the IOL implanted is a Light Adjustable Lens (RxLAL, RxSight), the opportunity for collaboration is even clearer. The optometrist has typically known the patient a lot longer than the ophthalmologist has. The optometrist knows the patient’s visual needs and personality better than the surgeon. If the surgeon is considering a monovision correction, the optometrist may be able to advise, having tried monovision contact lenses for the patient previously. If the patient did not do well with monovision contacts, the idea of monovision IOL correction can be dismissed.
A second opportunity for collaboration with the RxLAL is that the referring optometrist can see the patient before each of the planned light adjustments and demonstrate different visual options on the phoropter or with a contact lens trial. The patient can then be referred back to the ophthalmologist with his or her current prescription and an intended target. All the ophthalmic team needs to do is confirm the refraction and targets and then apply the light adjustment using the Light Delivery Device (LDD, RxSight).
The referring optometrist therefore shares in the decision-making process and the eventual determination of the refractive targets. The optometrist can levy a fee for this service, and the ophthalmologist levies a fee for the use of the LDD to adjust the IOL power. The RxLAL truly opens a new avenue for optometry and ophthalmology working alongside one another, both aligned to provide patients with the best possible outcomes.
BEYOND CATARACT SURGERY
This collaboration can extend beyond cataract surgery, too. Refractive surgery lends itself well to comanagement, and so does taking care of glaucoma and medical retina patients. The level of comanagement depends largely on the level of expertise present in the optometrist’s practice, what devices are being used, and whether the user has been properly trained to operate those devices and interpret the findings. Currently, optometrists who have access to devices such as OCT retinal imaging, corneal topography, and visual field analyzers are already proficient and using them in the referral process. It does not take much effort to raise their skills to the next level where treatment efficacy can be measured, and then patients can be referred for care with confidence. Additionally, the training in optometry courses is now at a much higher level than in previous decades. In some countries, optometrists can also further their knowledge by completing postgraduate courses and certificates in medical retina, glaucoma, and refractive surgery and in independent prescribing modules.
Training of the optometric referral base can also be undertaken by the ophthalmic practice. Providing clear guidelines on when patients require referral works in both the optometrist’s and the ophthalmologist’s favor, as both providers are relieved of having to see patients needlessly or redundantly. The further the relationship grows, the more the referring optometrists can start aligning their referrals with the ophthalmologist’s best practice standard operating protocols, the less often needless referrals are made, the fewer spectacles are erroneously prescribed, and the fewer cataract patients are sent home because their visual performance is simply still too good for surgery.
PROMISE OF NEW TECHNOLOGIES
Optometrists who do not have access to specialized tests can take solace in the fact that technologies are being developed that will provide optometrists and ophthalmologists with small smartphone-enabled access to Scheimpflug and Placido-disc images of the anterior segment for a monthly subscription fee, rather than the capital outlay needed to buy these devices. The resulting images, stored in the cloud, make comparisons between visits easier and allow more than one user to access the data. In this way, a topography performed by the optometrist 6 months earlier can be compared to today’s topography performed at the ophthalmologist’s office.
CONCLUSION
All the previous excuses for optometry and ophthalmology not to work together are diminishing. I predict that, in 10 to 15 years’ time, this model will be the way most eye care is delivered. Already, community-based schemes in Ireland, such as the Sligo Cataract Scheme, and in the United Kingdom show that this model helps clear patient waiting lists for surgery and streamline patient care. If this is the way it is going to be, why not be part of the evolution and write some of the guidelines that shape this collaboration? I’m not going to wait around. I want the best possible care for my patients today, and that includes having their referring optometrists be part of the surgical decision-making process and aftercare.
1.Global data on visual impairment. World Health Organization. http://www.who.int/blindness/publications/globaldata/en/. Accessed July 9, 2018.
2.Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: A Systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221-e1234.
3.Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systemic review and meta-anaylsis. Lancet Glob Health. 2017;5(9):e888-e897.
