



In the 15 years that I have been implanting intrastromal corneal ring segments (ICRSs) for keratoconus, I have learned a lot by experimenting with different models and strategies. The following list includes the top 10 pearls I have developed for successful ICRS implantation.

Ensure that the patient is a good candidate for ICRSs. This is probably the most important factor to avoid unhappy patients: Make sure the intervention is indicated before implanting an ICRS. It is important to determine the patient’s potential for improvement after surgery. For example, in some eyes with a small amount of ectasia, ICRS implantation can worsen the condition, and severe keratoconus can be unchanged or worsened after ICRS implantation.
One way to ensure patient candidacy is to use a rigid gas permeable (RGP) lens trial before electing surgery. If the patient experiences poor quality of vision or is intolerant of RGP lenses, ICRS surgery should be discussed as the only viable alternative to deep anterior lamellar keratoplasty (DALK). DALK is strongly recommended for patients with very thin (< 350 µm) or irregular corneas, or in eyes with central corneal scarring. ICRS implantation achieves the best results in keratoconus stages 2 or 3, or if significant anisometropia is present.

Explain the timeline, milestones, and limitations of ICRSs Patients must be informed that ICRS implantation is a biomechanical procedure that requires time—at least 3 months—to stabilize following surgery. Additionally, its effect can be further enhanced with follow-up or combined procedures such as CXL, excimer laser ablation, and IOL implantation. Before proceeding to surgery, patients must understand and accept the potential need for ICRS explantation or one or more of these adjunctive procedures.

Explain the need for combined procedures. It is difficult to discuss keratoconus surgery without mentioning combination strategies. In progressive keratoconus or for patients who rub their eyes habitually, combining CXL with ICRS implantation is a valuable option. CXL can be performed on the same day as implantation if the probability of success is high or if combined with topography-guided phototherapeutic keratectomy a few months after ICRS implantation in more challenging cases.

Perform adequate tomography and refraction. Refraction in patients with keratoconus is complicated because their visual quality is highly dependent on accommodation and light levels due to their extreme corneal varifocality. High levels of higher-order aberrations limit the reliability of aberrometry.
Nevertheless, one can obtain a reasonable estimate of the patient’s ametropia based on mean central keratometry and axial length. Keratoconus progression is based on corneal shape changes; therefore, corneal topography must be complemented with tomography, generally using Scheimpflug or OCT imaging technologies.

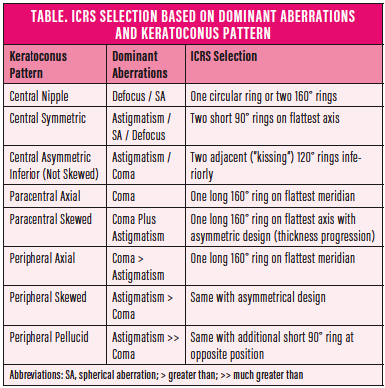
Define the dominant aberrations. It is often necessary to compromise and define an order of priorities for each individual. The most important areas to address are reductions in coma, astigmatism, defocus, spherical aberrations, and anisometropia. In some keratoconus patterns, coma and astigmatism can be easily addressed with one ICRS; others are more challenging. The information in the Table on the following page can help determine the best choice of ICRS based on the most dominant aberrations.

Choose the appropriate ring design. There are ICRSs of multiple lengths, thicknesses, and diameters to choose from. The number and diameter of segments is chosen based on the conus location; length is based on astigmatism; and thickness is based on the local keratometry. The steeper the cornea, the thicker the ring; the thinner the cornea, the thinner the ring. Compromises will sometimes be necessary.

Perform channel dissection with the appropriate tool. Femtosecond laser-assisted channel dissection is necessary to achieve perfect ICRS implantation. Placement of a calibrated incision on the steepest meridian with accurate centration, channel sizing, and depth is crucial for this surgery. In the event of corneal applanation, it is necessary to mark the center of the pupil; cyclotorsion can be managed with marks on the steepest axis for incision alignment.

Enhance ICRS positioning intraoperatively. Biomechanical response is not always predictable. Thus, fine-tuning the position of an ICRS should be undertaken during the procedure when needed. If possible, take into account the eyelid load and the interaction with the speculum by adjusting the ICRSs with the speculum removed, and dynamically assess their positioning during the blink process.

Enhance ICRS results postoperatively with complementary procedures. If corneal thickness is greater than 450 μm, topography-guided photoablation can be performed to improve visual acuity results. Transepithelial photoablation can be combined with mitomycin C and CXL if necessary. For patients with cataracts or high residual ametropia (defocus/astigmatism), phakic or pseudophakic IOL implantation can be an effective option.

Prevent eye rubbing, as extrusion of the implants is possible, allowing further progression. In patients with behavioral disease caused by their excessive eye-rubbing habits, education is important in order to avoid complications.
