


The use of intraoperative digital visualization can improve surgical accuracy and outcomes. My video shares advice for getting the most out of this technology (watch below).
FOUR PIECES OF ADVICE
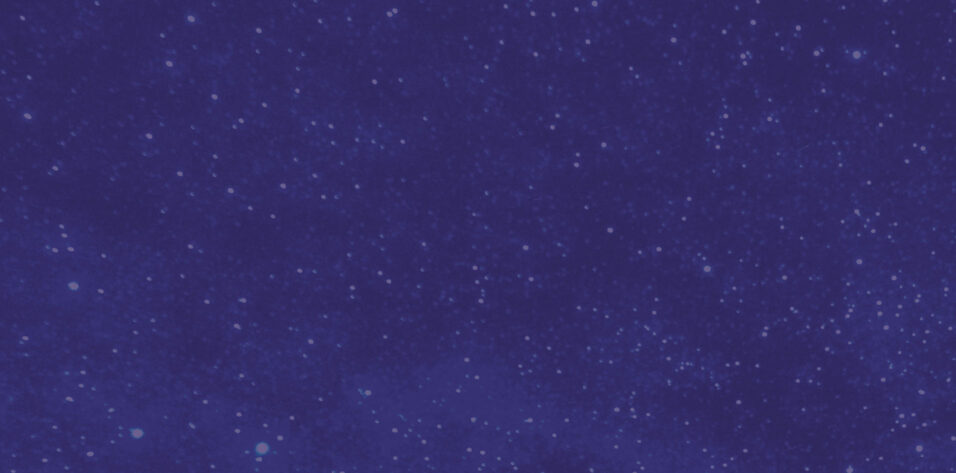
No. 1: Rely on iris registration. One of the most important components of intraoperative digital technology will be the advent of iris registration. Comparing the pre- and intraoperative eye will allow surgeons to quantitatively address several facets of surgery (Figure 1). These include steep axis and incision locations, toricity, and correct eye and laterality. Digital iris registration also permits the placement of digital marks and makes it easier for novice surgeons to find the paracentesis again during surgery (Figure 2).
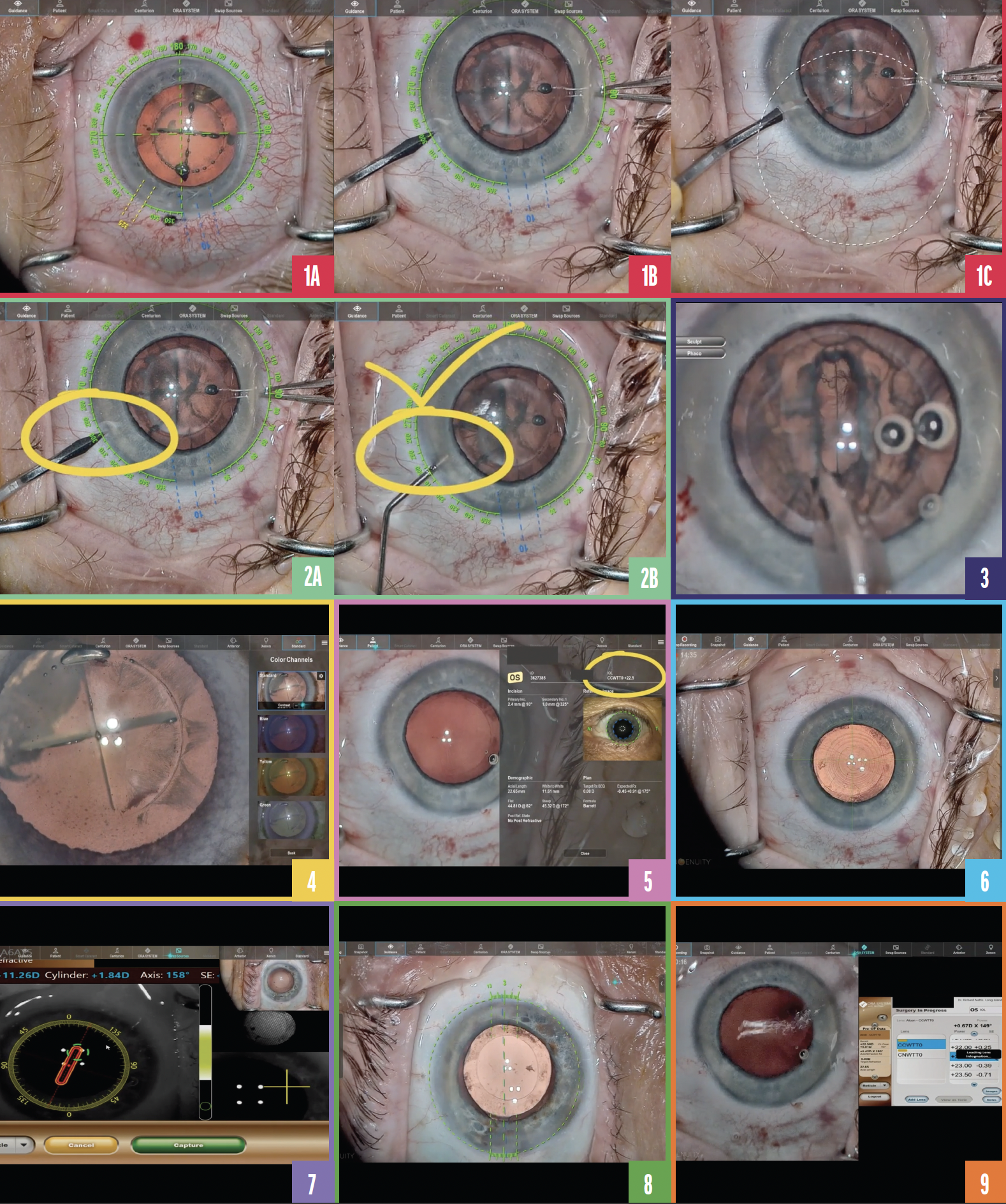
Figure 1. Various 3D views of the eye during surgery (A–C).
Figure 2. Digital iris registration marks simplify finding the paracentesis (A,B).
Figure 3. Improved visualization reduces the risk of complications. Detail and magnification are key.
Figure 4. The use of tissue detail mode facilitates an evaluation of capsular integrity and an incomplete laser capsulotomy.
Figure 5. The IOL selected based on preoperative biometry is crosschecked against the ORA calculation.
Figure 6. The toric IOL is aligned with the use of digital visualization.
Figure 7. Iris registration with 3D digital visualization.
Figure 8. A visual overlay of the toric axis and a picture-in-picture ORA representation are used to guide the placement and orientation of a toric IOL.
Figure 9. The view of the surgical field with 3D digital visualization.
No. 2: Enhance the surgical view. What can computers do that human eyes cannot? Digitally enhance and process images and video in real time. The high dynamic range camera on the Ngenuity 3D Visualization System (Alcon), for example, provides stereoscopic 3D imaging that performs area-specific sampling to minimize glare and shadows, enhance imagery, and provide unparalleled magnification. Detail and magnification are everything in ocular surgery, and the Ngenuity is capable of greater magnification than an analog microscope. Other 3D digital operative systems available include the Artevo 800 (Carl Zeiss Meditec) and Beyeonics One (Beyeonics).
Improve your visualization and decrease your rate of complications is a well-known adage (Figure 3). Tissue detail mode improves the surgeon’s ability to evaluate the integrity of the anterior capsule and laser capsulotomy (Figure 4).
No. 3: Perform crosschecks. Like pilots, ophthalmic surgeons rely on crosschecks. The Ngenuity integrates with the Argos Biometer With Image Guidance, ORA System, and VerifEye+ (all from Alcon). The system facilitates confirmation that the IOL on the tray matches the one selected preoperatively. It also facilitates a comparison of the preoperative biometry and intraoperative aberrometry measurements to help ensure that the optimal IOL power is chosen (Figure 5).
Intraoperative digital visualization allows the identification of angle kappa and alignment of incisions and presbyopia-correcting IOLs with the center of the limbus, pupil, or visual axis (Figure 6).
Digital visualization is particularly helpful with toric IOLs. Surgeons who operate with 3D visualization systems no longer need to spend time preoperatively approximating the 12, 3, 6, or 9 clock positions or worrying about cyclorotation of the eye (Figure 7). Ngenuity provides a digital overlay of the toric axis as measured from preoperative biometry and confirmed by intraoperative iris registration. This facilitates the accurate alignment of a correctly powered toric IOL (Figure 8).
No. 4: Keep your eyes on the prize. For years, I hated having to turn away from the surgical microscope to find the cart with the intraoperative aberrometer tucked in some corner of the OR. Heads-up surgery with a digital viewing system that integrates with an intraoperative aberrometer and phaco unit helps surgeons keep their focus where it should be: the surgical field (Figure 9).
