

Studies suggest that the age-standardized prevalence of myopia and hyperopia in Europe is 30.6% and 25.2%, respectively, with an increase in myopia anticipated.1 The worldwide prevalence of glaucoma is also increasing. In the future, more patients are therefore likely to have both glaucoma and refractive errors. What refractive surgical options are available to these patients?
CHOOSING THE BEST SURGICAL APPROACH FOR EACH PATIENT
A flowchart (Figure 1) can aid in selecting the appropriate refractive surgical method for an individual patient.

Figure 1. Flow chart for choosing the appropriate refractive surgical method.
Laser treatment. The first step is to determine if laser treatment is indicated. The applicable criteria for determining candidacy for laser procedures such as PRK, LASIK, and refractive lenticule extraction are the same regardless of whether a patient has glaucoma. The reliability of applanation tonometry after laser treatment, however, is a concern.
My colleagues and I measured biologically corrected IOP with the Corvis ST (Oculus Optikgeräte) in 200 eyes before and 3 months after SMILE treatment at the Center for Refractive Surgery in Münster, Germany, where I practice. We found that the average IOP reading was lower after surgery (Figure 2A). The reduction in corneal thickness, however, which was related to the thickness of the lenticule removed, was only weakly correlated with the decrease in IOP (Figure 2B), similar to after PRK or LASIK. Calculating the difference in IOP readings therefore does not appear to be feasible. As a result of our findings, we recommend adjusting the target IOP for glaucoma patients after refractive laser surgery based on several postoperative IOP measurements.
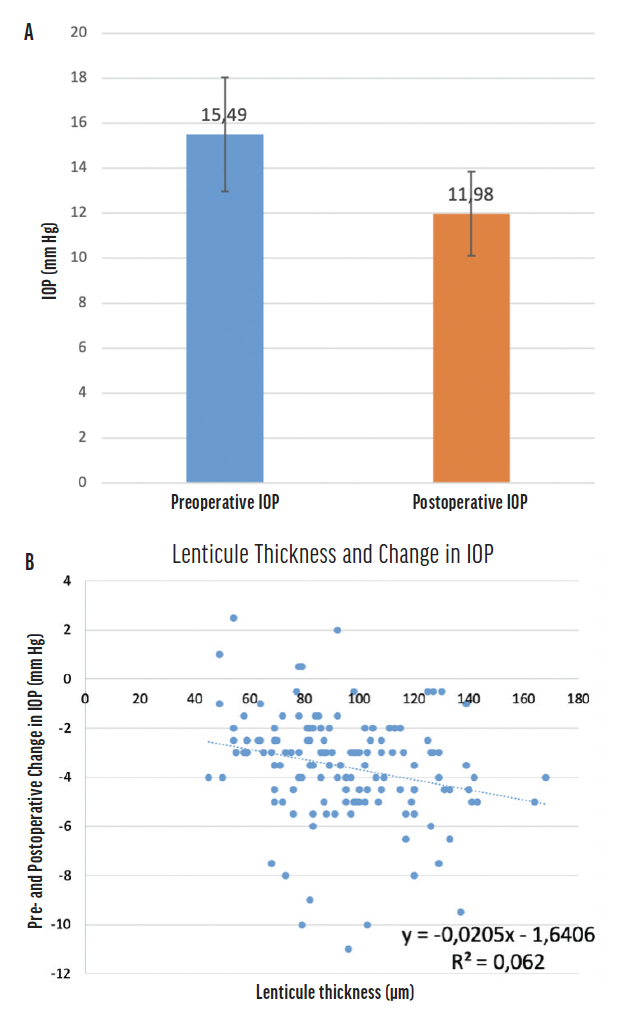
Figure 2. IOP before (blue) and after (orange) SMILE treatment (A). The study found a weak correlation between lenticule thickness and change in IOP (B).
Phakic IOL. If the patient is not a candidate for laser treatment, the next option to consider is a phakic IOL. This surgical intervention maintains the patient’s accommodative amplitude. The addition of central holes to modern phakic IOL designs for myopia correction has improved aqueous flow and rendered a preoperative laser peripheral iridotomy (LPI) unnecessary.
Our results with phakic IOLs such as the Visian ICL (STAAR Surgical) and Implantable Phakic Contact Lens V2.0 (Care Group) showed no clinically significant decrease in endothelial cell count or increase in IOP during the first 2 postoperative years.2 Our experience indicates that phakic IOLs are a reasonable option for correcting ametropia in patients with glaucoma. Proper patient selection, however, is crucial. The depth of the anterior chamber and size of the anterior chamber angle must be adequate to accommodate a phakic IOL.
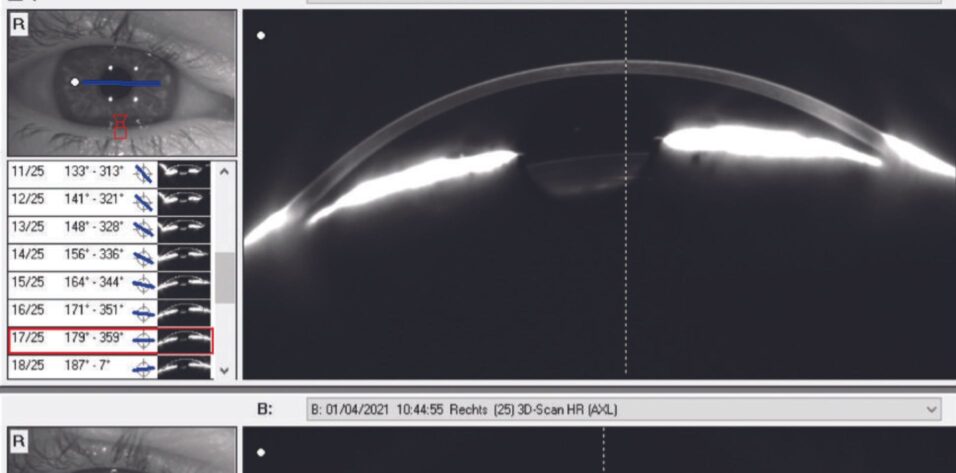
Refractive lens exchange. If laser refractive surgery and phakic IOL implantation are contraindicated, refractive lens exchange (RLE) may be an option for addressing refractive errors in patients who have glaucoma. We tend to choose RLE for presbyopic patients who have narrow anterior chamber angles, advanced glaucoma, and/or early cataracts. Replacing the crystalline lens with an IOL generally widens the anterior chamber angle (Figure 3). This can lower IOP and assist with glaucoma management, especially in patients with narrow-angle glaucoma.
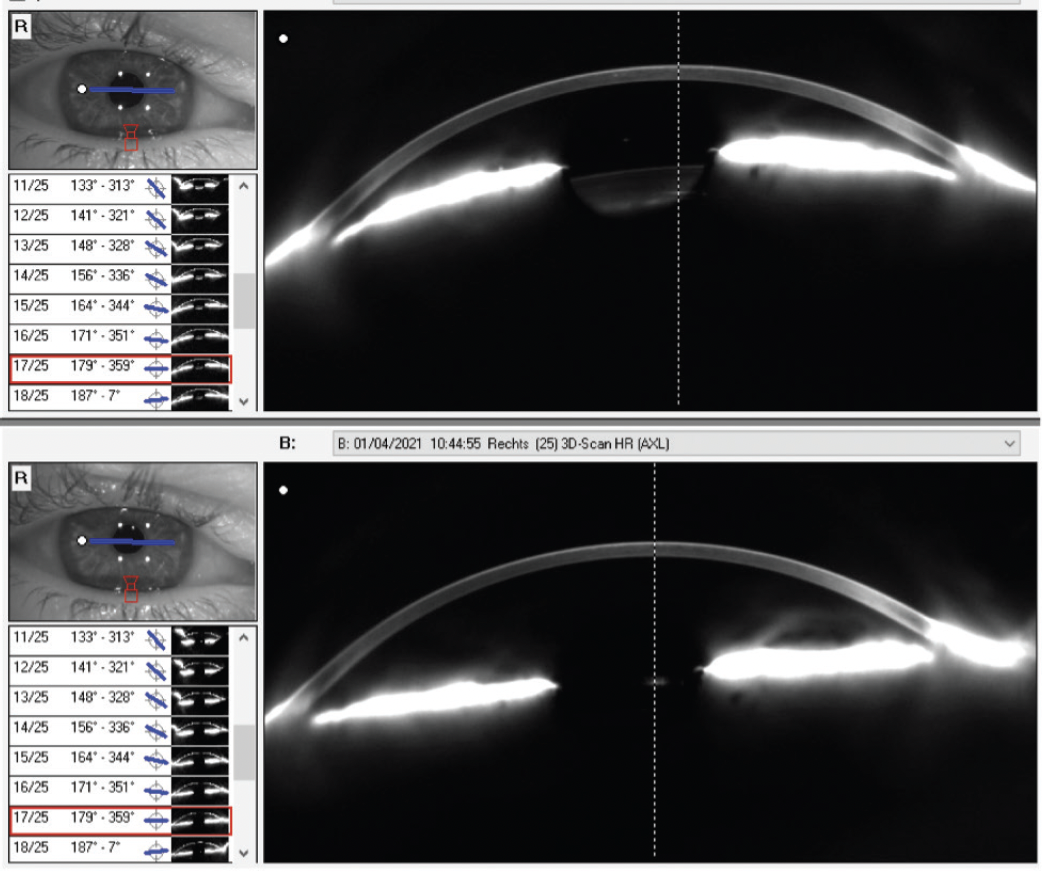
Figure 3. Scheimpflug image of anterior chamber before and after RLE. Anterior chamber angles of 23º preoperatively (top) and 45.9º postoperatively (bottom).
For years, the European Glaucoma Society has recommended RLE for the treatment of primary angle-closure glaucoma. The prospective, randomized, controlled Effectiveness of Early Lens Extraction for Treatment of Primary Angle Closure Glaucoma (EAGLE) trial compared RLE to LPI.3 In the study, RLE was more efficacious and cost-effective than LPI. In its current recommendations, the European Glaucoma Society reports a small but unequivocal superiority of RLE over LPI in all examined aspects.
Several factors, however, can make RLE challenging to perform. These include the presence of a narrow chamber angle, short axial length, flat anterior chamber, reduced endothelial cell density, pseudoexfoliation syndrome, narrow pupil due to treatment with pilocarpine eye drops, filtration bleb, and loose zonular fibers. Additionally, the effective lens position and postoperative refraction are less predictable in eyes with narrow-angle glaucoma compared to healthy eyes. Laser vision correction may therefore be required more often in glaucomatous eyes to achieve the target refraction.
CONCLUSION
Patients with glaucoma may have reduced contrast sensitivity or scotomas. These individuals can benefit greatly from refractive surgery that grants them independence from spectacles that distort or minify images.
1. Wolfram C, Hahn R, Kottler U, et al. Prevalence of refractive errors in the European adult population: the Gutenberg Health Study (GHS). Br J Ophthalmol. 2014;98(7):857-861.
2. Taneri S, Dick HB. Initial clinical outcomes of two different phakic posterior chamber IOLs for the correction of myopia and myopic astigmatism. Graefes Arch Clin Exp Ophthalmol. 2022;260(5):1763-1772.
3. Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomized controlled trial. Lancet. 2016;388(10052):1389-1397.
