



Various techniques and devices for cataract removal have been described and implemented worldwide. For more than 25 years, I have taught residents and fellows how to perform cataract surgery in what I consider to be the most safe and effective way. Cracking the nucleus successfully is one major hurdle that they must overcome. As I approach retirement, I have invested a lot of energy in training my successors, and I am happy with how they have mastered the basic principles of cataract surgery and minimized ineffective manipulations.
This article focuses on the essential mechanisms of manual cracking and how to execute this step in the simplest, most reproducible way.
SHARED TRAITS
All the residents and fellows I have taught learned cataract surgery elsewhere before coming to the Netherlands, where I practice. Their approach to cracking has been essentially the same, reflecting the traditional ideas behind the divide and conquer technique: Sculpt as deeply as possible before attempting a cracking maneuver.
The main drawback to sculpting nearly to the level of the posterior capsule is that inexperienced surgeons can become nervous during the last stage of deep sculpting. Their anxiety grows exponentially if the posterior capsule ruptures. The extreme stress the young surgeons feel stiffens their muscles, which generally reduces their level of control during manipulations.
THE MAJOR PRINCIPLES UNDERLYING SIMPLE, SUCCESSFUL CRACKING
No. 1: Crack at the point of greatest resistance. I recommend cracking the nucleus immediately after creating the first trench. The middle of the lens has the highest density and offers the most resistance to cracking, so focusing on this area minimizes the likelihood that the second instrument will slice through a softer part of the lens and fail to split the lens fibers. In my experience, this problem is far more likely to occur with the conventional technique of sculpting four trenches first and cracking thereafter. When the density of the nucleus is soft to medium, a lot of the trench walls may already be down, leaving little surface for successful cracking.
No. 2: Ensure the proper placement of the phaco tip and cracking instrument. Properly placing these instruments is simple to do but demands the surgeon’s focus and the right timing. When I am observing residents and fellows, it is often the case that one or both instruments are tilted upward slightly during the actual splitting action. This happens, I suspect, because young surgeons fear damaging the posterior capsule.
I find that hemi-cracking right after the creation of the first trench—which does not have to be ultradeep—with the phaco tip lightly pressed downward and the second instrument placed as deeply as possible results in a successful crack. Both instruments are gently pressed downward on the bottom of the groove (Figure 1). This may seem dangerous to a young surgeon, but it is not. Subsequent grooves are easier to crack because the first full split of the nucleus into two halves serves as a reference point. Again, the proper placement of the tip and second instrument is essential for additional grooves. Rotating the phaco tip clockwise to facilitate access to the bottom of the groove with the second instrument is a simple yet effective trick.
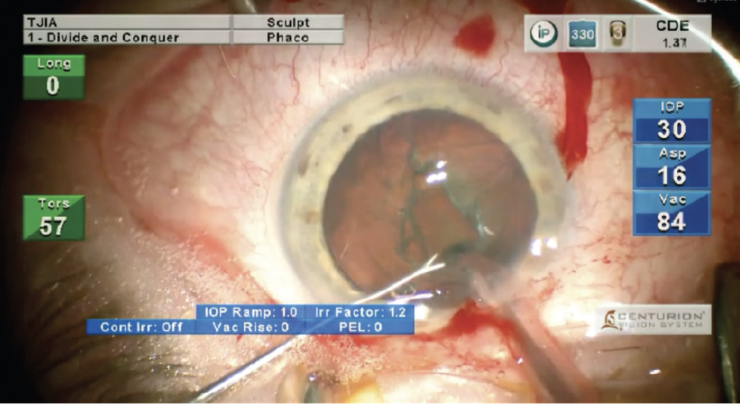
Figure 1. The instruments are placed at the bottom of the groove.
No. 3: Rotate the handle of the second instrument slightly to move it sideways. When the second instrument is located at the bottom of the groove, the surgeon can move it counterclockwise by lightly turning the handle between their fingers. Because the phaco tip is also positioned at the bottom of the groove, cracking the nucleus should require minimal movement (Figure 2).
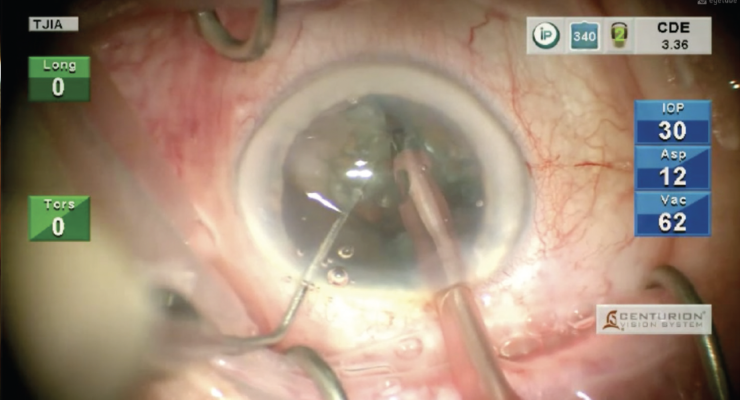
Figure 2. Cracking of the nucleus.
CONCLUSION
Provided the phaco tip and second instrument are held stable, cracking the nucleus should be an easy and reproducible maneuver if the three basic principles described in this article and demonstrated in the video are employed. In my experience, students learn these principles easily and gain confidence much faster than with the original technique of creating four grooves before cracking.
