



Femtosecond laser technology can help cataract surgeons customize their nucleus-cracking techniques, which can reduce phaco time, corneal endothelial cell loss, postoperative corneal edema, and the risk of rupturing the posterior capsule.1-4
LASER FRAGMENTATION
The type of cataract and degree of nuclear density are key determinants of the optimal phaco technique. The Lensar Laser System (Lensar) uses Scheimpflug technology for cataract imaging and automatically grades lens density on a scale of 1 to 5.5 The laser can be programmed to reflect the surgeon’s preferred pattern of phacofragmentation. The pattern is then automatically created and prepopulated on the system’s touchscreen for each case based on the cataract densitometry. This enables surgeons to evaluate the degree of nuclear density and type of cataract and disassemble the lens more efficiently. Surgeons can also change settings on the fly. For example, if I notice that the density of a lens is greater based upon densitometry than my clinical examination, I can alter the size of the capsulotomy after imaging and before performing the laser capsulotomy and fragmentation.
For soft nuclei, I use a pattern resembling four or six wedge-shaped pie cuts. For denser nuclei, I favor a grid-like pattern that cuts the lens into small cubes. I find this approach facilitates safe and efficient phacoemulsification with less nuclear manipulation and phaco power. Some surgeons have expressed concern that a fragment may get lost if the cube fragmentation pattern is used, but I have never experienced this problem.
The Streamline system can be used to create a customized capsulotomy with two small tabs or nubs at the axis of astigmatism for toric IOL alignment (Figure 1). There is also an option to automatically transfer astigmatism data from another diagnostic device such as the Cassini (i-Optics), Pentacam (Oculus Optikgeräte), or IOLMaster (Carl Zeiss Meditec).
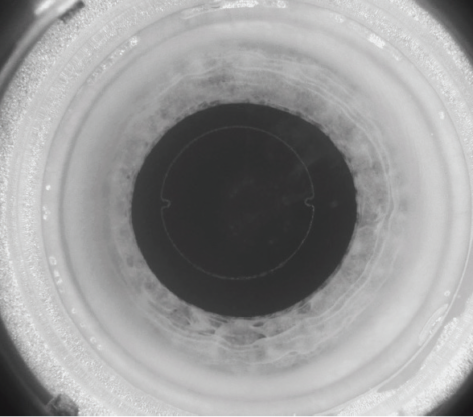
Figure 1. Astigmatism correction with a toric IOL using a femtosecond laser.
The capsulotomy is centered on either the capsular bag or the pupil, which can be especially helpful in patients with weak zonules or small pupils. In individuals with zonulopathy due to Marfan syndrome, trauma, or coloboma, the touchscreen can be used to move the capsulotomy that will be created into a better position and potentially place less stress on the zonules than a manual capsulorhexis.
CASE EXAMPLES
No. 1: Posterior polar cataract. These patients are usually young, and there is an increased risk of rupturing the posterior capsule due to inherent weakness or an opening in the posterior capsule. Imaging with a femtosecond laser system can sometimes reveal a ruptured posterior capsule.
Because posterior polar cataracts tend to be soft, I use a pie-cut fragmentation pattern. Gentle hydrodelineation of the lens is performed. An OVD is instilled, and the nuclear fragments are lifted and removed with minimal phaco power.
The area of weakness in the posterior capsule can be protected with hydrodelineation and by avoiding aggressive hydrodissection. It can be relatively easy and safe to viscodissect the lens fragments from the epinucleus. Some surgeons have expressed concern about rupturing the posterior capsule during laser cataract surgery on these eyes, but I have not encountered this problem.
No. 2: Dense cataract. I like to create multiple cuts in a cube-like pattern. All the cubes are removed by gently sculpting out a large bowl (Figure 2). When the epinucleus is reached, a small opening is created in it, or it is peeled away from the capsule. An OVD is instilled to viscodissect the leathery epinucleus from the capsule. This minimizes stress on the zonules and capsule. I avoid a blind chop, which increases the risk of posterior capsular rupture.

Figure 2. Laser cataract surgery on an eye with a grade 4+ white cataract. The cubed fragments are removed.
No. 3: Zonulopathy resulting from lens coloboma. In this situation, the use of a femtosecond laser permits the creation of a custom capsulotomy for a toric IOL with minimal zonular traction and a phacofragmentation pattern that corresponds to lens densitometry (Figure 3).
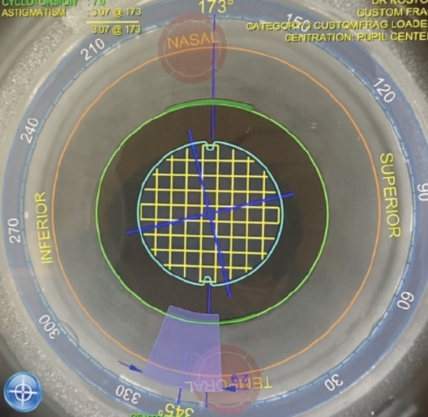
Figure 3. Fragmentation pattern used on a lens coloboma.
MANUAL TECHNIQUES
When cracking the nucleus manually, I choose my technique based on lens density and the type of cataract, as I do with femtosecond laser fragmentation.
For a routine cataract, a small groove is made, the lens is divided into hemi-nuclei, and each is chopped. For a dense lens, my first step is to determine whether the lens is mobile. A generous amount of OVD is instilled. In some cases, a bowl is gently sculpted to minimize trauma, debulk the nucleus, and remove the remainder of the lens material. Sometimes, I try to chop the nucleus depending on its density. In certain situations, I perform vertical chop.
CONCLUSION
Femtosecond laser technology can allow safe, consistent nuclear disassembly. Cataract density imaging helps to optimize the phacofragmentation pattern, minimize the amount of phaco power used, and provide predictable outcomes for patients.
1. Conrad-Hengerer I, Hengerer FH, Schultz T, Dick HB. Effect of femtosecond laser fragmentation on effective phacoemulsification time in cataract surgery. J Refract Surg. 2012;28(12):879-883.
2. Uy HS, Chan PS, Gil-Cazorla R, Shah S. Comparison of surgical parameters using different lens fragmentation patterns in eyes undergoing laser-assisted cataract surgery. Int Ophthalmol. 2019;39(11):2459-2465.
3. Al-Mohtaseb Z, He X, Yesilirmak N, Waren D, Donaldson KE. Comparison of corneal endothelial cell loss between two femtosecond laser platforms and standard phacoemulsification. J Refract Surg. 2017;33(10):708-712.
4. Scott WJ, Tauber S, Eck CD, Scott RA, Ohly J. The clinical relationship of anterior capsular tears and vertical spacing in the femtosecond laser capsulotomy procedure. J Refract Surg. 2019;35(5):280-284.
5. Donaldson K, Fernández-Vega-Cueto L, Davidson R, et al; ASCRS Refractive–Cataract Surgery Subcommittee. Perioperative assessment for refractive cataract surgery. J Cataract Refract Surg. 2018;44(5):642-653.
