


Whether dividing, chopping, fragmenting, or flipping a nucleus, I focus on ensuring adequate capsular coverage of the IOL, gently performing surgery, and minimizing phaco energy. I am always ready to change course depending on the specific situation.
MY GO-TO TECHNIQUE
I favor a divide and conquer technique combined with a little phaco chop. Where I practice in Minnesota, I regularly see patients with pseudoexfoliation, so I make minimizing stress on the zonules and capsular bag complex a priority.
A corneal marker is used to outline a centered, 5.2-mm capsulorhexis. Part of my modified divide and conquer technique involves creating a fluid wave with hydrodissection. Without rotating the nucleus, a groove is created in the center of the cataract (Figure 1), and a second instrument is used to divide the nucleus in half. With the phaco probe, a second sideways groove is then made in the first hemi-nuclear piece. Next, the first quadrant is divided with a chopper and removed without rotation (Figure 2). The second quadrant is then rotated to the iris plane and removed. The remaining hemi-nuclear piece is grabbed at the distal end and chopped to avoid maneuvers close to the endothelium.(See below for a video demonstration.)
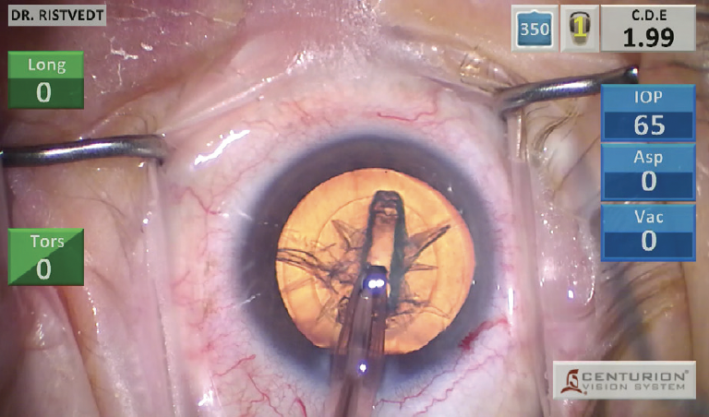
Figure 1. A groove is created in the center of the cataract.
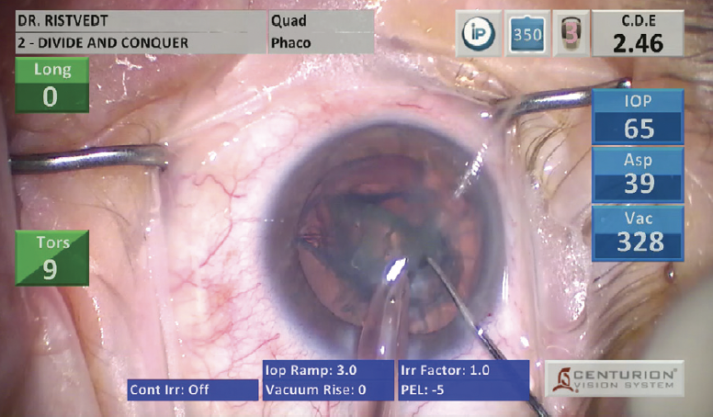
Figure 2. After the first quadrant is divided with a chopper, it is removed without rotation.
In my hands, this technique is a quick and energy-efficient way to remove the nucleus, regardless of its density.
ADJUSTMENTS
Preferences aside, in some situations, I find it helpful to adjust certain steps of nuclear disassembly.
Brunescent cataracts. Instead of making a central groove, I use a miLoop (Carl Zeiss Meditec) to divide brunescent cataracts so that I can avoid creating and managing a posterior plate. (See below for a video demonstration of surgery with the miLoop.) The key to getting comfortable with the miLoop is to practice on cataracts that allow the device to be visible as it passes under the nucleus (Figure 3). Only then should one proceed with operating on eyes where that visual cue is absent. After the cataract has been divided in half, it can be rotated and split again with the miLoop.
Figure 3. The miLoop passes under the nucleus.
With a second instrument, each hemi-nucleus is brought to the iris plane and chopped into multiple pieces, and each piece is aspirated. The more fragments that can be created without the use of phaco energy, the quieter the eye will be postoperatively.
Manual small-incision cataract surgery. This approach can be valuable for cases in which a high amount of phaco energy is required and the cornea may recover more slowly or decompensate as a result. Learning manual small-incision cataract surgery has given me the confidence to operate in areas of the world where patient access to care and the availability of modern technology are limited. (See below for a video demonstration of manual small-incision cataract surgery.) The key is to make a proper scleral tunnel with dissection into the cornea at the same plane. The incision is longer on the inside of the corneal incision and shorter externally where the scleral groove is started. In many cases, the capsule must be stained with trypan blue dye, or a can-opener technique must be used to avoid posterior capsular openings. The nucleus is gently rotated out of the bag. Under visualization with a lens loop, the cataract is expressed with posterior pressure and a fluid wave.
CONCLUSION
Knowing when to deviate from my preferred fragmentation technique and being comfortable performing a variety of strategies to crack the nucleus help to ensure safe surgery every time.
