



Choice of phaco technique depends on a surgeon’s personal preference, the technology available, and the patient’s ocular anatomy and pathology. The two most common techniques are divide and conquer and phaco chop. The latter, introduced by Nagahara in 1993 at the American-International Congress on Cataract, IOL, and Refractive Surgery in Seattle, is my preferred method to crack the nucleus.
During chopping, the lens is broken bimanually into several fragments with the help of a second instrument, such as a Nagahara chopper. The phaco tip is inserted into the lens core. The chopper is then carefully placed under the lens capsule and pulled from the periphery to the phaco tip. This splits the lens into two pieces. Because the movement is mainly horizontal, the technique is also called horizontal chop (differentiating it from vertical chop, which is addressed in the accompanying sidebar).
PHACO CHOP IN 11 STEPS
No. 1: Check the sleeve. When the sleeve of the probe is correctly positioned on the phaco handpiece, the irrigation holes are horizontal, and both irrigation and phacoemulsification are functional. This can be confirmed by briefly pushing the footpedal before entering the eye.
No. 2: Insert the phaco tip. The phaco tip is inserted into the anterior chamber with the help of the chopper to keep the corneal incision open.
No. 3: Remove the superficial epinucleus. The superficial epinucleus is extracted by rotating the opening of the phaco tip downward and performing careful aspiration.
No. 4: Stabilize the core. The phaco tip is inserted paracentrally into the lens on the side of the main incision until the entire tip is embedded in the lens core. With sufficient vacuum, the phaco tip can now hold the core in place.
No. 5: Insert the chopper. The chopper is inserted with the tip oriented horizontally under the lens capsule and opposite the main incision.
No. 6: Rotate the chopper. The instrument is rotated so that its tip is aligned vertically.
No. 7: Establish counterpressure. The chopper is pulled toward the phaco tip to create slight counterpressure with the phaco handpiece.
No. 8: Bisect the cataract. Just before the two instruments touch, the chopper is used to pull the nucleus to the left and the phaco tip is used to push the opposite half of the lens to the right. This splits the lens.
No. 9: Further divide the nucleus. The footpedal is set to irrigation, the lens is rotated, and steps No. 4 through 8 are repeated to fragment the lens further. Four, six, or even eight (if the lens is particularly hard) fragments are created.
No. 10: Emulsify the fragments. Each fragment is pulled individually into the center of the anterior chamber and onto the iris plane with the phaco tip and emulsified. Before removal of the final fragment, the tip of the chopper is rotated upward and positioned underneath the phaco tip so that the instrument can help to prevent capsular rupture (Figure 1).
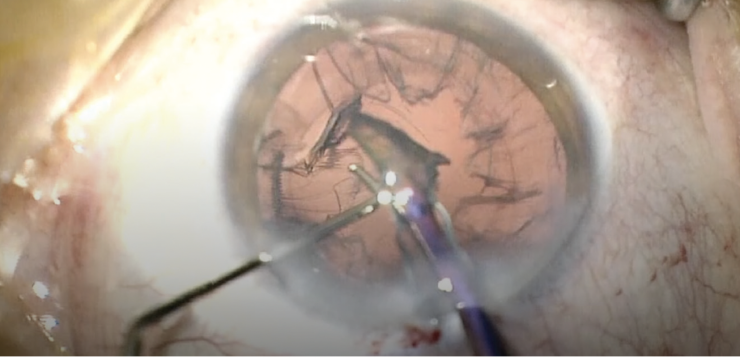
Figure 1. The chopper is placed underneath the last fragment to reduce the risk of a posterior capsular rupture.
No. 11: Remove residual epinucleus. Any remaining epinucleus is mobilized with the second instrument and removed with aspiration.
ADVANTAGES
The phaco chop technique is particularly useful for eyes with hard lenses and weak zonules because little ultrasound energy is required for fragmentation of the lens and minimal shearing forces act on the zonular apparatus. During the chopping maneuver, the vacuum level should be high, and ultrasound energy should be low and set to burst mode.
To remove the fragments, the vacuum level is reduced, and aspiration and ultrasound energy are increased. Ultrasound is set to either pulse or continuous mode (the latter is suitable for experienced surgeons). Some surgeons favor dual-linear control with the footpedal for phaco chop because it allows vacuum and ultrasound energy to be used in a highly controlled manner.
VARIATIONS ON THE TECHNIQUE
Stop and chop. This technique combines aspects of the divide and conquer and phaco chop techniques. An initial groove is created as it would be with divide and conquer. The lens is divided into two pieces, which are subsequently split into smaller fragments with the phaco chop technique.
Phaco quick chop (also known as vertical chop). The lens is pulled upward with high vacuum. A pointed chopper is pressed into the lens and pulled toward the phaco tip, thereby pulling apart the nucleus. This technique is not suitable for soft lenses.
PITFALLS
Because phaco chop is a bimanual technique, the initial learning curve can be steep. Typical chopping mistakes by beginners include the following:
No. 1: Shallow penetration of the cataract. If the phaco tip does not reach an adequate depth in the nucleus, countertraction with the chopper may be too feeble to allow splitting of the lens.
No. 2: Insufficient vacuum. If the vacuum is too low, then it can be difficult to achieve stable fixation of the lens.
No. 3: Incorrect movement of the chopper. Guiding the chopper vertically to the periphery may lead to accidental damage of the anterior capsule when the instrument is pressed against the lens. Alternatively, if the instrument is not advanced far enough into the periphery, then proper pressure cannot be applied to the lens; instead of splitting the nucleus, its surface may only be scratched (Figure 2).
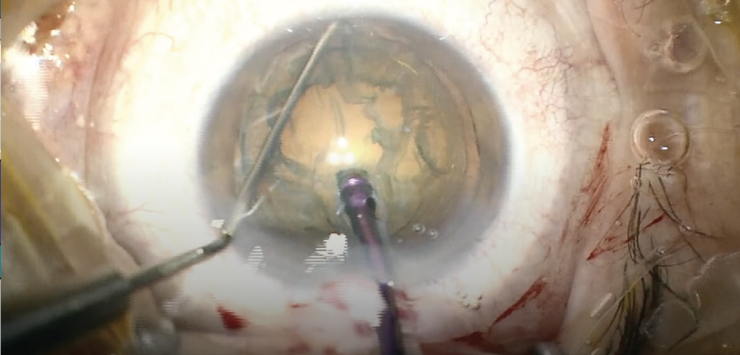
Figure 2. The chopper has been moved well beyond the capsulorhexis and into the periphery to promote division of the lens.
No. 4: Poorly positioned chopper. If the tip of the chopper points downward as the final lens fragments are removed, movement of the posterior capsule during aspiration through the phaco tip may bring them into contact and rupture the capsule. To prevent this complication, the tip of the instrument should be in a horizontal orientation whenever it is not being used.
No. 5: Overly high settings. If the aspiration rate or ultrasound energy level is too high, fragments may be aspirated instead of held by the phaco tip.
No. 6: Too much pressure on the sideport and main incisions. This can increase leakage of anterior chamber fluid and make chopping much more difficult.
CONCLUSION
Once mastered, phaco chop can offer surgeons flexibility and allow rapid removal of almost any type of cataract while minimizing stress on the zonular apparatus.
Read more about the steps of cataract surgery in Dr. Shajari’s book, Cataract and Lens Surgery.
