


EyeTelligence
Mark Lobanoff, MD

Every cataract patient has a journey that takes them from the clinic for preoperative assessment to the OR to recovery. As surgeons, our job is to safely and skillfully guide patients on that journey to their best possible vision. Digital technology such as EyeTelligence (Bausch + Lomb) can assist us every step of the way. Watch a promotional video below.
PATIENT JOURNEY STEPS
Preoperative assessment. At the preoperative visit, patients undergo tests such as topography, macular OCT, wavefront analysis, and biometry. A tremendous amount of data is generated—often more than we can analyze before meeting patients to discuss IOL options. EyeTelligence can help by analyzing the data and providing the details we need to counsel them. For example, the software can alert us to a high angle alpha or kappa via an app on our smartphone so we can take the information into account if considering a multifocal or extended depth of focus IOL. Similarly, the software can alert us to a high root mean square, indicating a high magnitude of higher-order aberrations. EyeTelligence also analyzes anterior corneal topography and can alert us if asymmetric or irregular astigmatism is found.
Surgical planning. The data generated during testing are used to populate IOL formulas. Entering data manually is time consuming and introduces the chance of transcription errors. EyeTelligence automatically stores and organizes data in the cloud. It displays astigmatic data from different devices for easy comparison. The platform also harvests information (eg, allergies, medications, comorbidities) from the electronic health record (EHR) system. We may choose from among our favorite IOL formulas or use the EyeTelligence Assistant, which evaluates the eye’s unique physical characteristics, compares them to a database of 30,000 eyes, and determines which IOL formulas should be most accurate for a given eye (Figures 1 and 2).
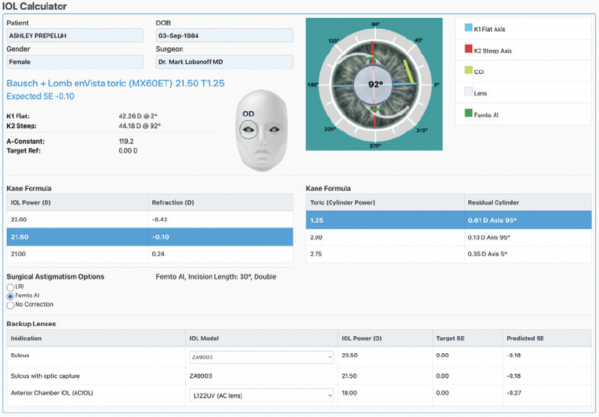
Figure 1. An EyeTelligence cataract surgery plan (fictional patient information).
Figures 1–3 courtesy of Bausch + Lomb
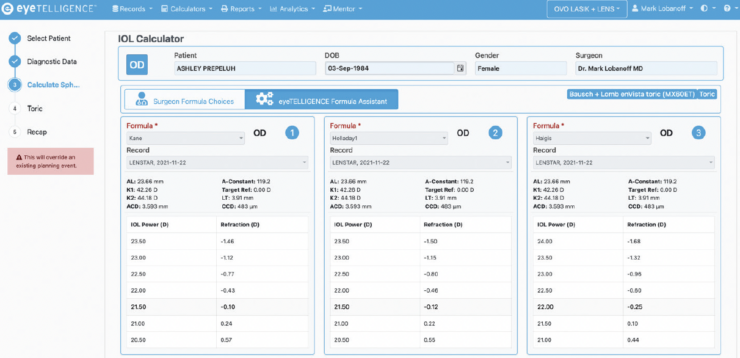
Figure 2. The EyeTelligence Formula Assistant advises surgeons on which IOL formula might be the most accurate for a given eye (fictional patient information).
In the OR. Staff can scan a patient QR code and the barcode on the IOL box with the EyeTelligence phone app to determine if the correct patient and IOL are in the OR (Figure 3). This can help prevent errors, which may occur despite rigorous checks instituted by the surgeon and staff.
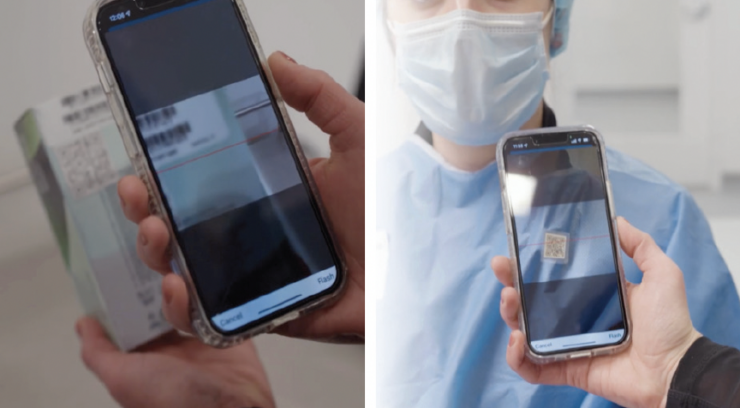
Figure 3. The EyeTelligence phone app is used to scan the patient’s QR code and the bar code on the IOL box.
Postoperative care. A busy surgeon often completes 16 or more cataract cases per surgery day. The day after surgery, they could spend 30 minutes tracking down patient results in the EHR system and calling comanaging optometrists. Alternatively, the surgeon could consult the EyeTelligence app on their phone, which can show instantly which patients are doing well and which may need closer follow-up. In this way, EyeTelligence can increase practice efficiency.
Smart Solutions
John A. Hovanesian, MD

Many of the diagnostic instruments and therapeutics that ophthalmologists use today are nothing like those they used 25 to 30 years ago. One process that has not changed significantly during that time, however, is IOL selection. Many cataract surgeons take a printout from their biometry system and circle a lens power. Alternatively, information from a biometer is entered into a website to calculate a lens power. In other words, an inefficient analog system prone to error is still the norm.
Fortunately, digital systems are emerging to modernize IOL selection. An example is the digital planner SmartCataract from Alcon. The company is developing a digital portfolio called Smart Solutions to integrate with a comprehensive equipment portfolio for the clinic, OR, and support services.
HOW DIGITAL PLANNERS WORK
SmartCataract was designed specifically for ophthalmology. It can integrate with multiple clinical diagnostics and EHR systems like NextGen Healthcare’s that we use in my practice to consolidate all my relevant data in one place and enable remote cloud-based planning. Patient data are populated throughout the planning process. The latest IOL formulas are available, and my personal preferences and settings are used to drive lens selection (Figure 4).
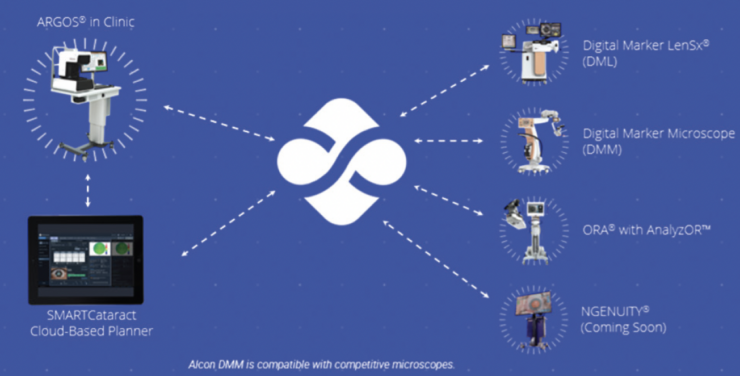
Figure 4. Diagnostic devices connect with SmartCataract to streamline cataract planning workflow.
Courtesy of Alcon
My staff and I can leverage our biometer, ophthalmic microscope, laser cataract system, and intraoperative aberrometer for image guidance and the transfer of patient data. Integration is not limited to Alcon hardware; diagnostic equipment from other manufacturers is also compatible.
WHY SWITCH TO A DIGITAL SYSTEM?
Something I like about remote planning is the instantaneous availability of information in SmartCataract to every stakeholder in the system. Not having to transfer paper plans to my ambulatory surgery center has streamlined planning so that it is rarely necessary to ship IOLs overnight for surgery—a real economic benefit. The technology also reduces stress on my staff; they are no longer under pressure to enter data manually into online calculators or machines, which is a process prone to error.
Surgeons regularly seek ways to optimize pre- and postoperative workflow, improve efficiency, and reduce transcription and other errors. An integrated, digital surgical planner can move patient information seamlessly, removing multiple points of manual data entry and saving considerable time.
The software, moreover, continues to improve. Manufacturers regularly enhance their systems based on surgeon feedback. Companies in- and outside of ophthalmology are collaborating to bring together the best in digital security and scalable technology. The future of digital solutions in ophthalmology is exciting.
Zeiss Cataract Workflow
Nicole R. Fram, MD

Digitally integrated workflow was only a dream even 2 years ago because of the need for USB plugins for data privacy and Health Insurance Portability and Accountability Act (better known as HIPAA) compliance, unreliable reference images, cost-prohibitive technology, and other issues. Barriers remain, and it can be challenging to convince a surgery center or hospital to purchase a nonreimbursable technology. Increased efficiency, reduced errors, and improved patient outcomes are the strongest arguments for investing in a digital surgical suite.
The first positive step toward digitally integrated workflow was the development of biometers that could provide advanced reference images with more reliable keratometry. Next, affordable, technology-agnostic digital workflow software helped surgeons abandon wasteful, bulky paper charts and increase efficiency in IOL planning and outcomes tracking. It is now an incredibly powerful time to be a cataract surgeon. A digital OR is like a fully integrated cockpit, with a microscope that integrates digital marking for incision placement, orientation to the optical axis, centering and sizing of the capsulotomy, and astigmatism management. My contribution to this article focuses on the Zeiss Cataract Workflow (this and all other devices referenced in the remainder of the article are manufactured by Carl Zeiss Meditec).
I find the best way to describe workflow with Zeiss’s digital suite is to consider a typical patient experience. The patient arrives for a preoperative evaluation that includes biometry, corneal topography, and tomography before the administration of topical drops. Data from the IOLMaster 700 and reference image are sent directly to the Veracity Surgical Planner (Figure 5). Corneal topography and tomography and additional biometry measurements can be integrated with the system. The information needed to plan cataract surgery, including IOL type, refractive target, postrefractive surgery status, the latest IOL formulas, toric and relaxing incision calculators, the Barrett Integrated K formula for anterior keratometry, and operative notes, are all available with the click of a button (Figure 6). There is no need for recalculations if the target refraction or IOL is updated, and separate websites for toric IOLs and limbal relaxing incision calculations are a thing of the past (Figure 7). Lastly, the IOLMaster reference image is sent to the OPMI Lumera 700 microscope for digital marking of the axis of astigmatism during surgery (Figure 8). Feedback on phaco parameters and video integration/editing with the Quatera 700 phaco system are on the horizon (Figure 9). Finally, the postoperative refraction is entered into Veracity with an integrated EHR, and the outcomes are analyzed and reported.
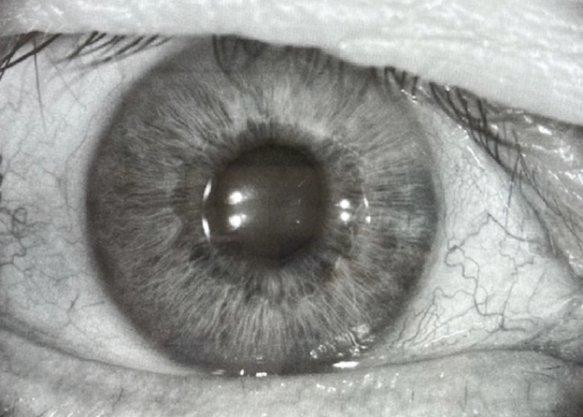
Figure 5. A reference image from the IOLMaster 700 is used to identify the steep axis, scleral vessels, and iris features.
Figures 5–9 courtesy of Nicole R. Fram, MD

Figure 6. IOL power calculation with Veracity Planning Software. The lens type, target refraction, and latest IOL formulas are available.
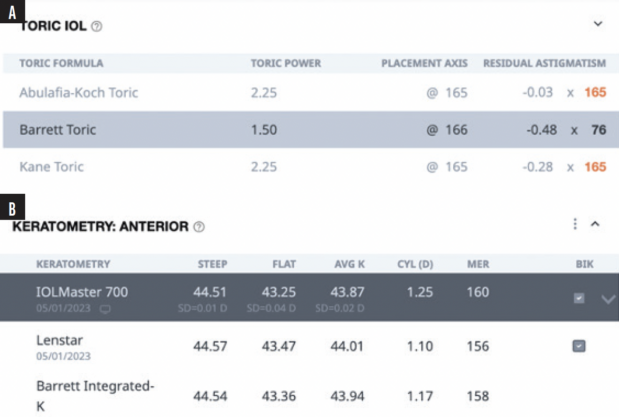
Figure 7. Toric IOL calculators (A) and the Barrett Integrated K formula (B) are integrated into the Veracity Planning Software.
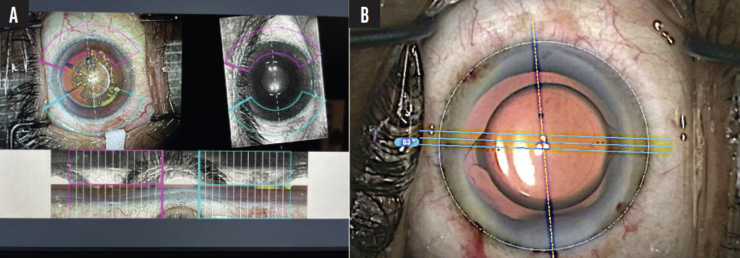
Figure 8. The reference image is confirmed on Callisto Eye (Carl Zeiss Meditec; A) and integrated into the microscope for toric IOL alignment on the steep axis (B).

Figure 9. Integration of Callisto digital marking and Quatera phacoemulsification with video recording.
The digital integration to improve the surgical planning workflow, efficiency in the OR, and the accuracy of IOL planning has become a reality.
Editor’s note: The content in this article was compiled before Cassini announced the launch of its digital cataract surgery suite technology, Cassini Connect. For more information on the platform, visit https://cassini-technologies.com/news-cassini-connect/
