



Analog surgical visualization allows ophthalmologists to perceive ocular tissues in a familiar and natural way, akin to diagnostic modalities such as slit lamps, fundus cameras, and anterior segment photography. It can be useful, however, to highlight certain details or imaging data embedded within a digital color image. This becomes possible, even in real time, with technology that uses digital filters to modify the regular microscope view.
DIGITAL FILTERS
The creation and application of digital filters rely on simultaneous contrast. This principle involves the combination of complementary colors to enhance contrast in an image. Contrast is often thought of in relation to black and white, but this specifically refers to light-dark contrast, one of seven types of contrast (Figure 1). These seven variants are the main instruments for creating digital filters for particular surgical scenarios.
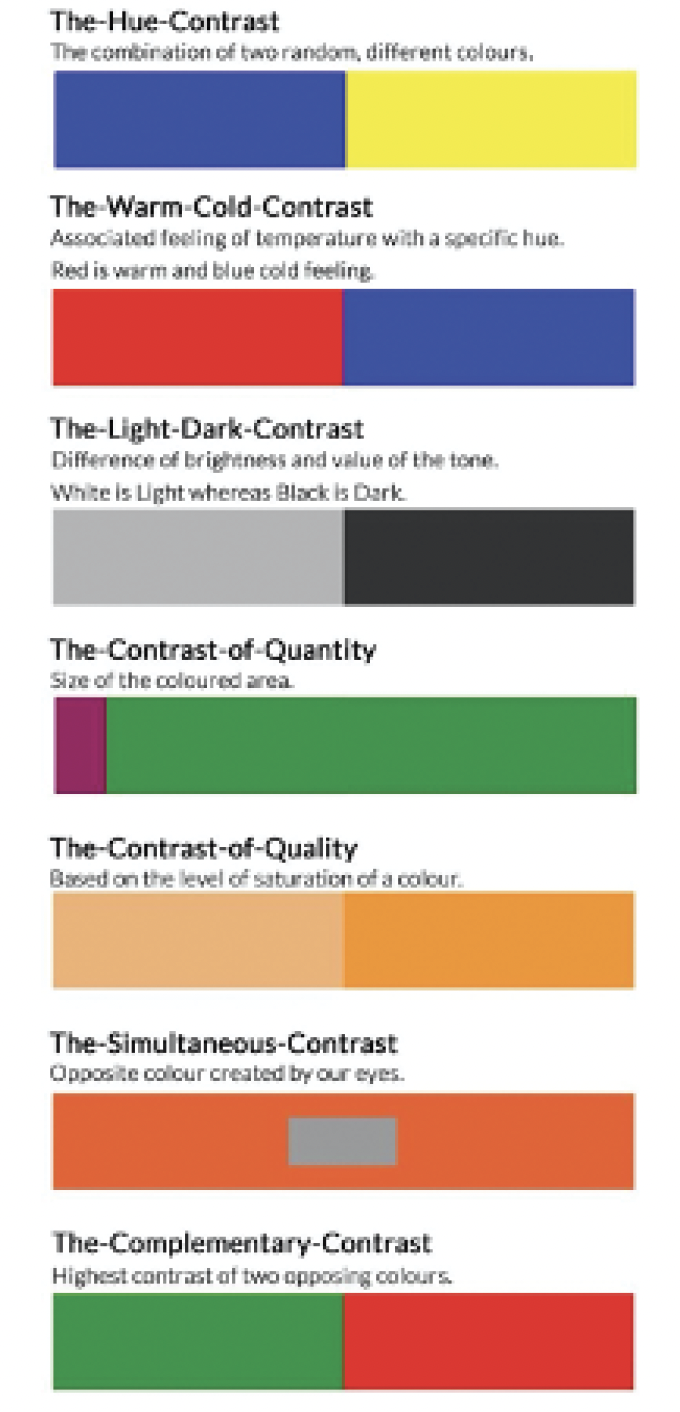
Figure 1. The seven types of contrast.
Over the past 2 years, I have created a few filters on the Ngenuity 3D Visualization System (Alcon) that I have found beneficial in my routine anterior and posterior segment surgeries. My approach has been to modify multicolored specifications rather than create monochromatic modifications. Adjusting more than one color allows me to utilize the composite image data in a digital color image fully and take advantage of the different types of contrast. (Click here to see the various filters applied during surgery.)
Fundus enhancement filter. I have found this filter facilitates the capsulorhexis by highlighting the fundus reflex in eyes with different types of cataracts, opacities, and even mild hemophthalmus in the posterior pole. The filter also improves visualization during hydrodissection and hydrodelineation. Moreover, it maintains the transparency of the nuclear pieces after chopping and during phacoemulsification (Figure 2).
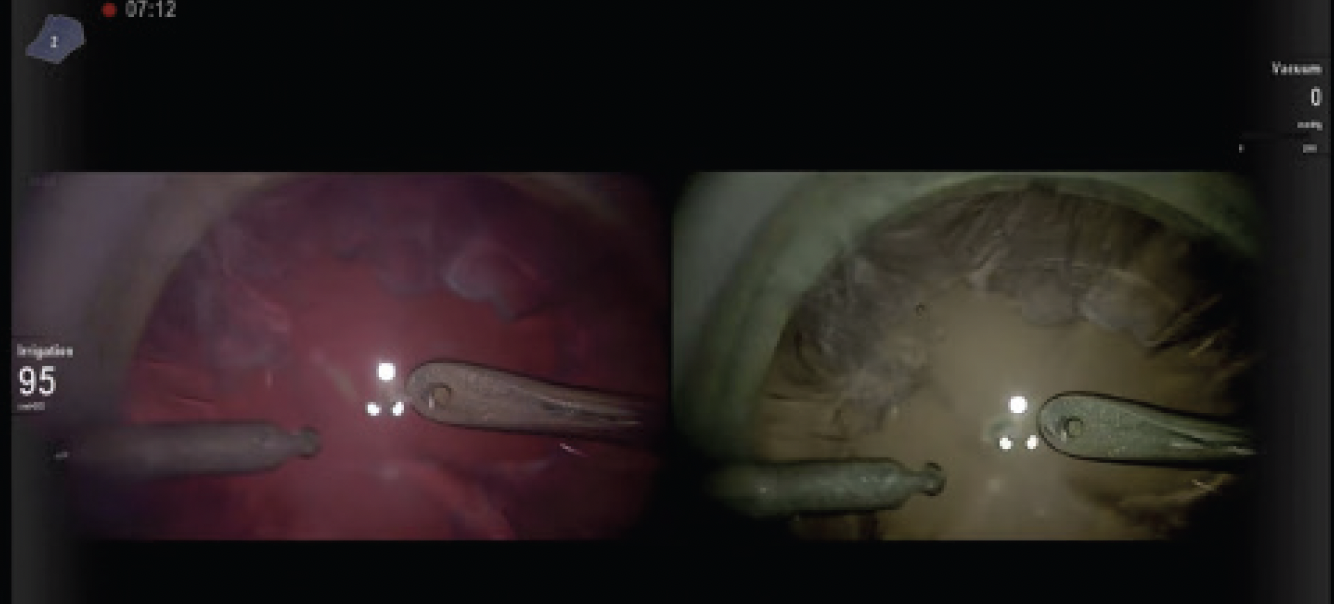
Figure 2. Application of the fundus enhancement filter during surgery.
Contrast enhancement filter. When applied during irrigation and aspiration, this filter increases contrast between dark and light areas, thereby improving my ability to distinguish between tissues of similar transparency (Figure 3A). For example, the filter aids in distinguishing the lens capsule from the cortex by highlighting the capsular edge, folds, and cortical remnants.
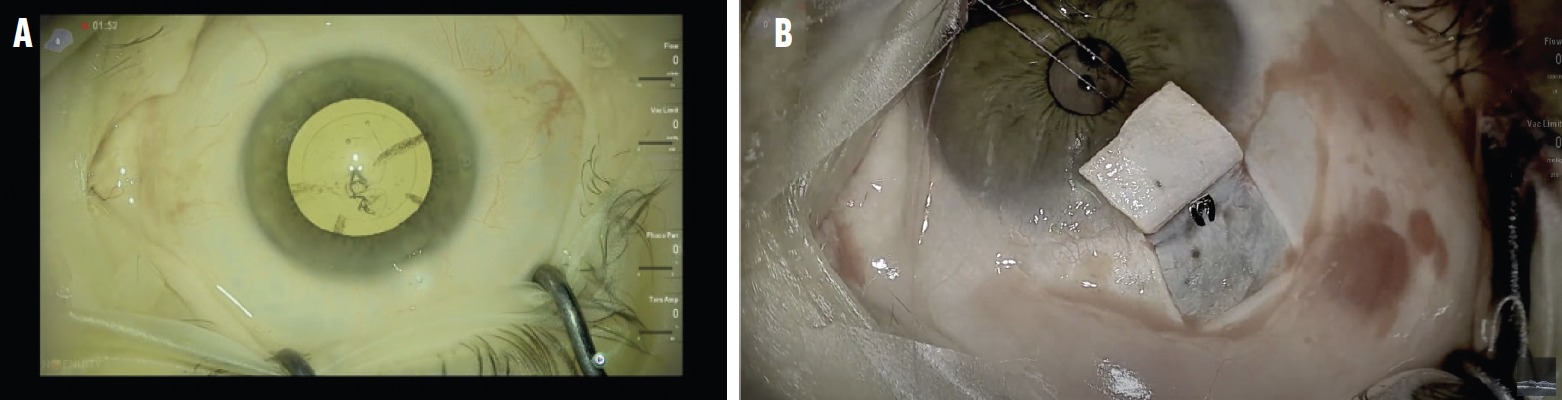
Figure 3. Application of the contrast enhancement filter during surgery to improve Dr. Mishev’s ability to differentiate between tissues of similar transparency (A) or reduce the graphic appearance of blood (B).
The filter can also be used to render the appearance of blood less graphic during procedures such as trabeculectomy or the creation of scleral pockets (Figure 3B). Using the contrast enhancement filter during goniosurgery can improve visualization of the angle structures (Figure 4).
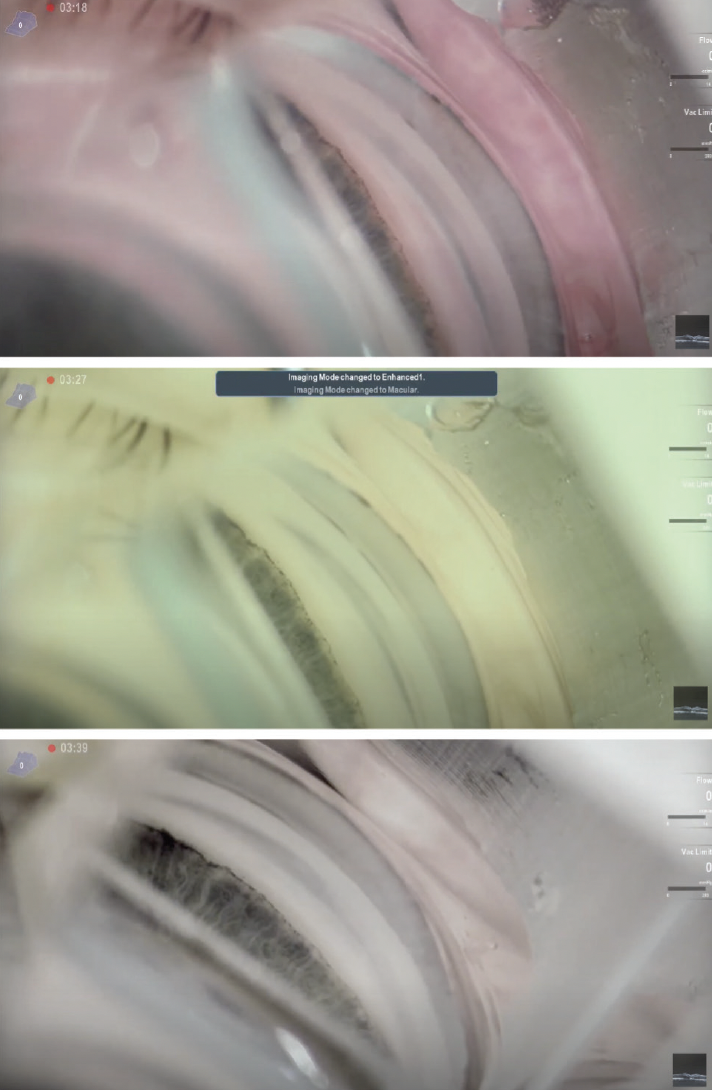
Figure 4. Using the contrast enhancement filter during goniosurgery improves visualization of the angle structures.
Autofluorescent filter. This filter provides fluorescent imaging of the conjunctival and scleral vessels. Its application during angle-based glaucoma surgery allows me to observe the blanching phenomenon that signals working filtration (Figure 5).
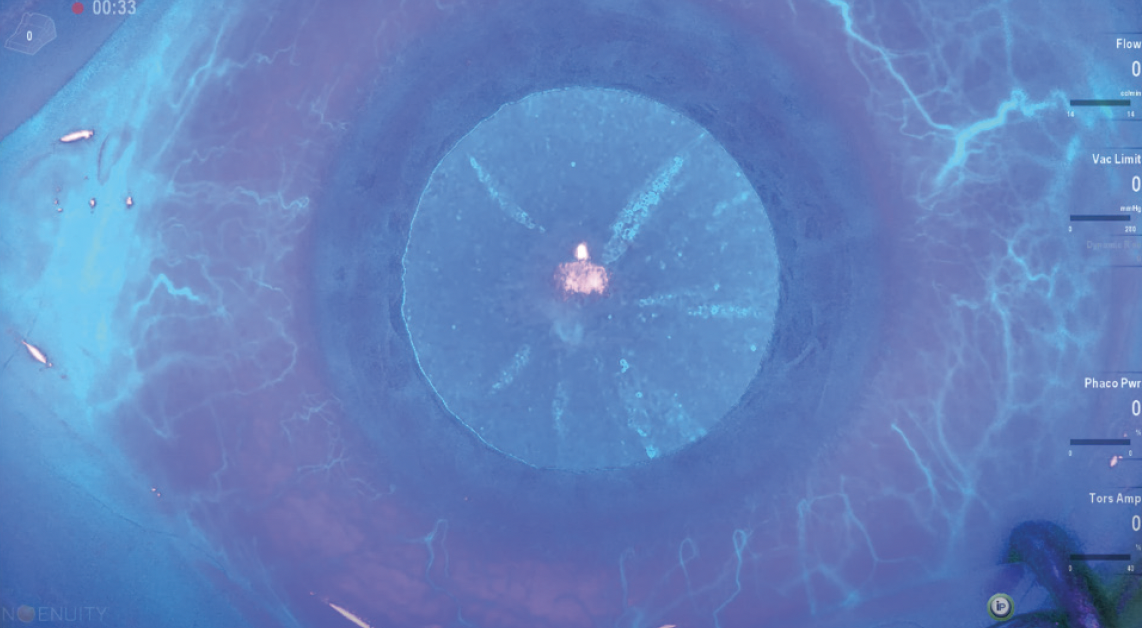
Figure 5. The autofluorescent filter provides fluorescent imaging of the conjunctival and scleral vessels.
TWO ADDITIONAL IMAGING MODALITIES
Two more imaging modalities can be achieved with the Ngenuity by using additional illumination sources on the microscope (Figure 6) and a dedicated digital filter to capture the fluorescence.
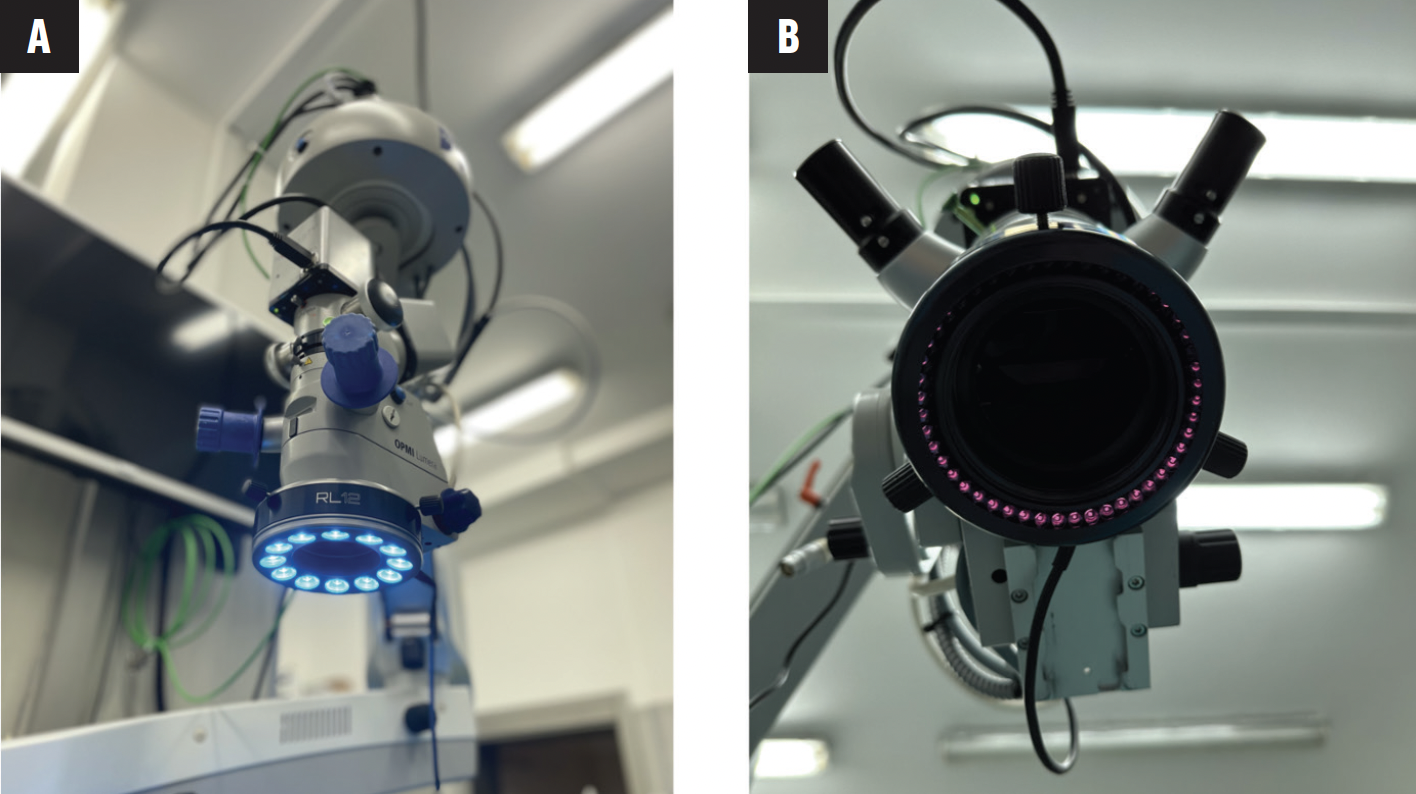
Figure 6. The Opmi Lumera (Carl Zeiss Meditec) with 475-nm (A) and 755-nm (B) LED rings.
Intraoperative fluorescein angioscopy of the anterior segment. This imaging modality requires a 475-nm excitation light source and either intravenous (500 mg/5 mL) or intracameral fluorescein solution 0.01%. No hardware barrier filter is required to visualize the fluorescence because a custom, proprietary filter on the Ngenuity captures the fluorescence. This is the main difference between the digital visualization system and a classic fundus camera. Also, intraoperative diagnostic and navigational data can be viewed in real time.
Intraoperative fluorescein angioscopy can provide useful information on the location and functionality of the collector channels. This information can influence where angle-based intervention (ie, implant, goniotomy, sclerostomy) occurs in eyes with pseudoexfoliative glaucoma, aid the evaluation of aqueous outflow after a filtration procedure, and facilitate the assessment of clinical complications such as capillary hemorrhage, blood-aqueous barrier defects, pseudouveitis, and anterior chamber hypoxia (Figure 7).1
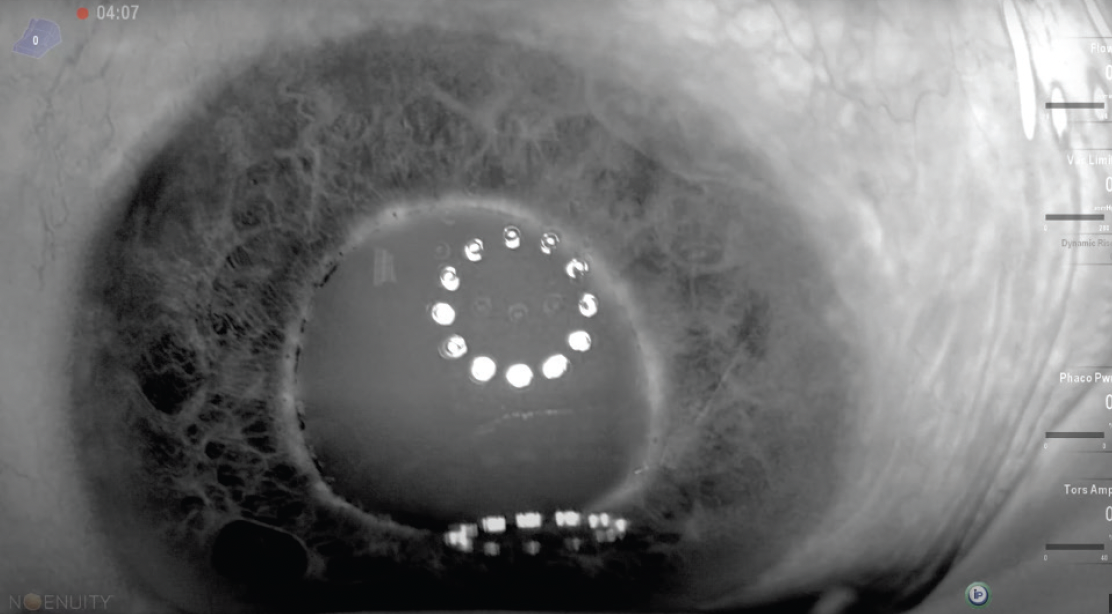
Figure 7. Intraoperative fluorescein angioscopy.
Infrared meibography. This imaging modality is achieved with the Ngenuity, an infrared 755-nm light source mounted on the microscope, and a dedicated digital filter (Figure 8).
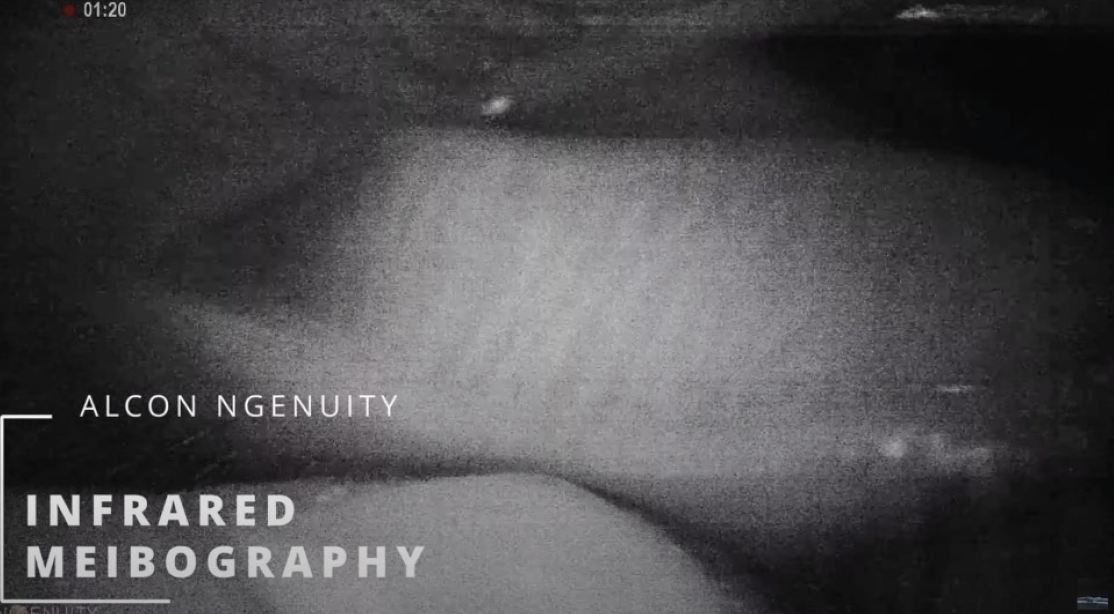
Figure 8. Infrared meibography.
CONCLUSION
In the future, it may become possible to filter a specific area of interest. In other words, a zone could be filtered to highlight the tissue or landmark of interest, and the rest of the image would be represented in regular color. This could improve discrimination by maximizing our useful image perception. Currently, we must change the overall surgical field, highlight certain areas of interest, and use image data in others. For example, in fundus enhancement mode, the fundus, capsulorhexis, and nuclear fragments are highlighted, but image data in the limbus and cornea are lost, making it difficult to create corneal incisions.
One approach would be to create a drag-and-drop tool with predetermined or adjustable shapes (ie, circle, arc, rectangle) that can be placed on the area of interest. The tool would have all available digital filters preprogrammed for selection based on the situation and which area should be filtered. The intensity of the filter should also be adjustable to allow quick transition from a regular to a filtered image at the spot of interest. The area-of-interest filter could be paired with a limbus-tracking algorithm to maintain the position where the tool is dragged and dropped.
1. Schlötzer-Schrehardt U, Naumann GOH. Ocular and systemic pseudoexfoliation syndrome. Am J Ophthalmol. 2006;141(5):921-937.
