

Microinstruments enable surgeons to competently and confidently perform complex ophthalmic surgical procedures without distortion and collapse of the eye. Micrograspers and microforceps, for example, are specifically designed to allow structures to be manipulated through microincisions (ie, 0.9-mm paracenteses) in anterior segment surgery. These tiny instruments provide excellent visualization of anterior chamber details without compromise and with a low risk of chamber collapse and endothelial damage.
One surgical procedure that can involve a high degree of intraocular manipulation is IOL exchange. This article outlines the advantages of using microinstrumentation for complex lens exchange procedures.
AT A GLANCE
•The growing use of premium lenses has led to an increase in the number of IOL exchange procedures.
• There is a need for instrumentation that enables safe and reproducible IOL exchange surgery.
• Available microinstruments include forceps, graspers, and scissors that allow controlled lens exchange and promote excellent recovery and predictable refractive and visual outcomes.
TECHNIQUE
I use two 0.9 paracentesis incisions and a 3.0-mm incision for lens removal and implantation in IOL exchange procedures. I start off by making the paracentesis incisions and then inject a dispersive OVD; my preference is Viscoat (Alcon). The anterior chamber is filled with the OVD, displacing the aqueous. I use a little pressure to ensure that the dispersive OVD adheres to the endothelial surface.
I then use Ahmed micrograsper forceps (MicroSurgical Technology [MST]) to lift the edge of the anterior capsule. Entry of the instrument allows egress of some OVD and reduction of chamber pressure. With the anterior capsule grasped and lifted, I insert the cannula underneath and inject more OVD to distend the anterior capsule. Then, advancing the cannula toward the equator, I inject more OVD very slowly, hoping to see a wave of the viscoelastic material behind the lens optic dissecting it away from the capsule. Further OVD injection at the site of each haptic eventually results in the isolation and dislocation of the lens within the capsule bag. With lenses that have been in place for a long period of time (4 years or more) and those with closed loops, the process can be more challenging; however, it can be accomplished with some perseverance as well as gentle and repeated viscodissection.
As long as the posterior capsule is intact, lenses with closed-loop haptics can be dissected using serrated blade forceps (micro-holding forceps [MST]), which are used to hold the lens haptic, to enable gradual injection of OVD underneath and toward the equator, and at the same time, to tease and ease out the haptic (Figure 1). If there is a dense adhesion present in, for instance, a closed-loop haptic lens, the haptic can be cut and rotated out.
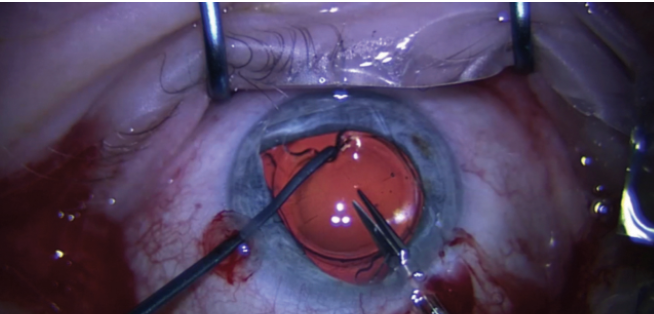
Figure 1. Micro-holding forceps are used to handle an implanted IOL intended for exchange.
Once the lens is dissected out and mobile, it is rotated if necessary, and the superior haptic is prolapsed into the anterior chamber. More OVD is injected to distend the capsular bag, with special emphasis at the equator 90° away from the location of the haptics to enable implantation of a CTR (Ophtec). If the CTR goes out to the equator and is not caught by an adhesion between the anterior and posterior capsules, I am reassured that an IOL can be implanted within the capsular bag.
With the superior haptic of the existing IOL prolapsed, I then implant the new lens behind the old one and into the capsular bag. Inserting the new implant before cutting and removing the old implant makes for much safer surgery. This method has the advantages of keeping the anterior segment formed and providing a barrier to prevent inadvertent involvement of the posterior capsule during bisection and removal of an old haptic or optic.
To cut the lens, Packer/Chang IOL cutters (MST) are inserted through the main incision, taking care not to involve the iris posteriorly and also avoiding contact with the cornea anteriorly. If the old IOL is a closed-loop lens, the superior haptic is cut first, followed by the optic, leaving the inferior haptic loop intact. One half of the superior haptic and optic are then grasped with the serrated micrograspers and gently removed. Another instrument is held with the left hand to control the movement of the remaining lens parts, avoiding damage to anterior segment structures including the cornea. The remaining portion of the lens is rotated, and the second half of the optic is regrasped to enable easier removal.
Watch it Now
IOL Exchange for a Trifocal Lens Implant

ADDITIONAL APPLICATIONS
The MST instruments described in this article for IOL exchange surgery can be used for many other anterior segment procedures as well, including repositioning and suturing of lens implants, transscleral externalization of lens haptics for glued IOL fixation, goniosynechiolysis, and iris suturing. Intraocular suturing can also be accomplished using specially made needle holders and Ahmed microtying forceps (MST).
CONCLUSION
The value of performing surgery through small incisions and keeping the chamber formed is well accepted, but developing devices to accomplish this task is challenging. The availability of these instruments designed specifically for anterior segment use has revolutionized anterior segment surgery and expanded previous surgical boundaries. I highly recommend the microinstruments described herein to all anterior segment surgeons who wish to perform challenging anterior segment surgical procedures.
Sheraz M. Daya, MD, FACP, FACS, FRCS(Ed), FRCOphth
• Director and Consultant Surgeon, Centre for Sight, East Grinstead, United Kingdom
• Chief Medical Editor, CRST Europe
• sdaya@centreforsight.com
• Financial disclosure: None
