



Management of keratoconus, a disorder characterized by progressive corneal thinning, has improved thanks to the availability of numerous treatment modalities including toric phakic IOLs, CXL, and PRK. Another helpful technology is intrastromal ring segments (ICRSs), which can play their part to decrease refractive error and improve corneal surface regularity by reducing the steepness of the central cornea.1 ICRSs may be used alone or in combination with PRK and/or CXL, depending on the severity of corneal ectasia and the patient’s visual needs.
There are a number of ICRS devices on the market. I use the Keraring (Mediphacos), which was specifically designed to treat corneal ectasia. The original Keraring is available in two models (SI-5 and SI-6) for implantation at optical zone diamters of 5.0 (SI-5), 5.5, or 6 mm (SI-6). Keraring ICRSs are available in 40 variations of thickness, arc length, and diameter. At the end of 2015, the company also introduced gradient thickness, asymmetric ICRS designs (150–250 and 200–300 μm) indicated for treatment of asymmetric keratoconus cases with the so-called duck, snowman, and croissant phenotypes.
NEW CONCEPT IN CORNEAL RESHAPING
Recently, Mediphacos developed an entirely new corneal ring to treat corneal ectatic disorders. Known as the Keraring Second Generation (SG), this new device is based on a unique concept for actually reshaping the cornea. In the past, our approach was to select an ICRS according to thickness, in order to reduce refractive error and improve corneal regularity. With the Keraring SG, the aim is to create the ideal corneal curvature with the use of a double-ring segment. The Keraring SG produces the ideal curvature by using peripheral remodelling, which flattens the central cornea and rebuilds corneal asphericity. Because of the double-ring element, the Keraring SG can remodel a wider area of the cornea than the traditional single-element Keraring.
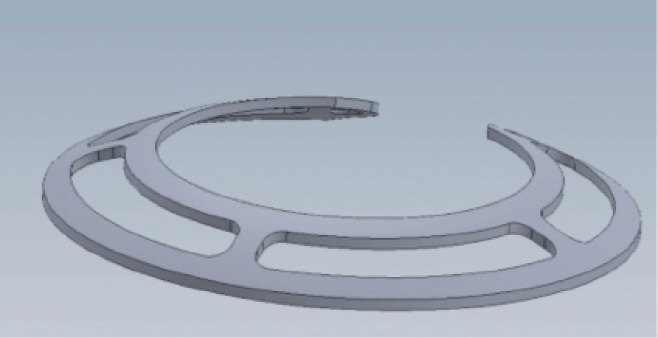
Figure 1. The 330º Keraring SG.
The Keraring SG is available in two models: a 330° segment (Figure 1) and a 160° segment (Figure 2). Both models consist of two segments joined by several bridges to produce a double arc. Each model is available in curvatures of 30.00, 35.00, 40.00, and 45.00 D. The objective in choosing which of these double-segment elements to use is to select the ideal one to produce an ideal curvature. The 330° segment is suited to patients with central nipple keratoconus or a bow-tie cone with low astigmatism. For patients with higher astigmatism (>2.50 D), inferior cone keratoconus, or post-LASIK ectasia, I would choose a 160° segment.
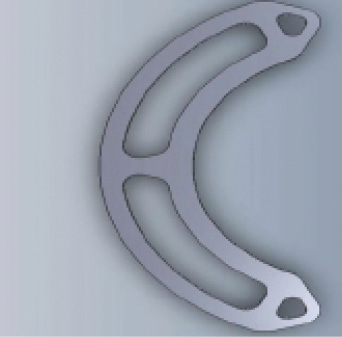
Figure 2. The 160º Keraring SG.
For example, if I have a patient with central nipple keratoconus with low astigmatism and a corneal curvature of 45.00 D, I would use a 330° segment—either 35.00 or 40.00 D—to create a flattening effect, which, in turn, will help to improve the patient’s refractive outcomes based on preoperative manifest spherical equivalent refraction.
For implantation of the Keraring SG, I prefer to use a femtosecond laser to create the intrastromal pocket. This is because the device is a wide segment, and also because, for this particular type of ICRS, it is unnecessary to create tight channels to accomplish the corneoplasty effect, as with standard or single-element ICRSs. I recommend creating a femtosecond pocket with an inner diameter of 4.7 mm and an outer diameter of 8.4 mm at 70% corneal depth.
CASE STUDIES
I have implanted several Keraring SG ICRSs in patients with keratoconus and post- LASIK ectasia. Below I share results in three patients.
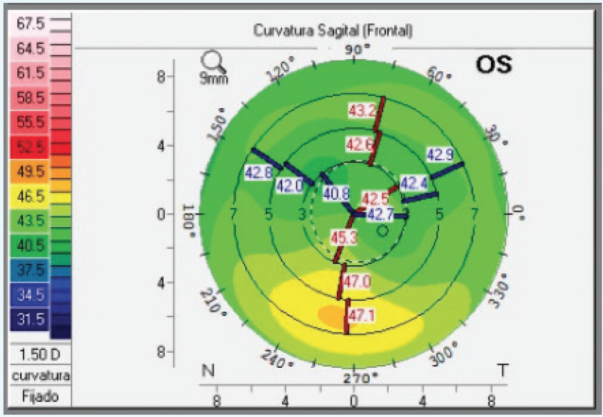
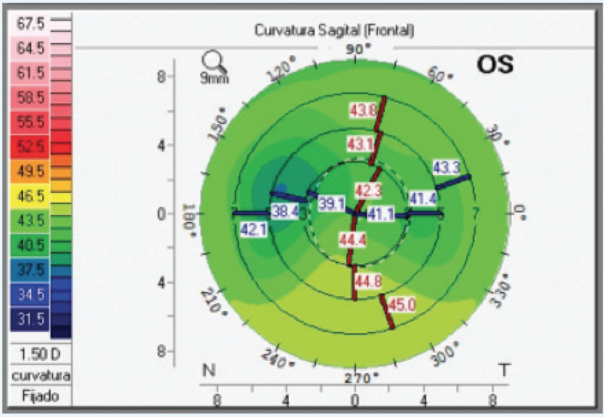
Figure 1. Pre- (top) and postoperative (bottom) sagittal maps show topographical improvement in inferior keratoconus. Corneal regularity improved after a single Keraring SG 160º, 40.00 D inferior implantation.
Case No. 1: A patient with inferior cone keratoconus presented with UDVA of 20/50, CDVA of 20/25 D, and refraction of +1.50 -1.00 X 180º. The patient’s corneal thickness on pachymetry was 465 µm, and Z3 horizontal coma as measured by Pentacam (Oculus Optikgeräte) Zernike analysis was -1.312 µm. One month after implantation of a single 160°, 40.00 D Keraring SG, the patient achieved UDVA and BDVA of 20/25 and 20/20, respectively, and his refraction was 0.00 -1.25 D X 165º. The patient’s astigmatism and pachymetry remained about the same as preoperative, and Z3 horizontal coma improved to -0.487 µm (Figure 1).

Figure 2. Single 160°, 40.00 D Keraring SG implanted inferiorly. The corneal flap can be seen surrounding the Keraring SG margin.
Case No. 2: A patient with post-LASIK ectasia presented with CDVA of 20/100, BDVA of 20/40, and -2.50 D astigmatism. The patient’s refraction was +0.75 -2.50 X 175º. Pachymetry was 482 µm, and Z3 horizontal coma was -0.918 µm. Seven days after a single 160º, 40.00 D Keraring SG was implanted inferiorly (Figure 2), UDVA was 20/40 and CDVA was 20/25 with a refraction of 0.00 -1.00 X 160º. The patient’s astigmatism was -1.00 D, pachymetry was 501 µm, and Z3 horizontal coma was -0.351 µm (Figure 3).
Case No. 3: A patient who presented with central nipple keratoconus had a UDVA of counting fingers and CDVA of 20/40. The patient’s refraction was -4.00 -1.75 X 60º with astigmatism of -1.75 D; pachymetry measurement was 482 µm. At 1-month postoperative, UDVA and CDVA were 20/40 and 20/30, respectively, and refraction was 0.00 -2.00 X 25º. Astigmatism was -1.75 D, and pachymetry was 471 µm.
Figure 3. Pentacam Zernike analysis pre- (left) and postoperatively (right). Postoperative Zernike shows general improvement, and Z3 horizontal coma was reduced from -0.918 to -0.351 μm.
CLINICAL STUDY FINDINGS
Eliane Nakano, MD, at the Escola Paulista de Medicina, in Sao Paulo, Brazil, is conducting an ongoing study to investigate the effects of the Keraring SG 330º in 40 eyes of 40 patients. Eyes in the study are subdivided into groups according to preoperative maximum keratometry (Kmax). Group A includes eyes with a Kmax of up to 60.00 D, and group B includes eyes with a preoperative Kmax between 61.00 and 75.00 D. A single 330° arc or two 160° arcs, depending on the amount of corneal astigmatism, are implanted in each study eye. All arcs have 45.00 D curvature.
Six-month postoperative follow-up data, available for
29 eyes of 29 patients (11 implanted with the 330° Keraring SG and 18 with two 160° Keraring SGs), showed continual improvements in UDVA and CDVA throughout the follow-up period (Figure 3).
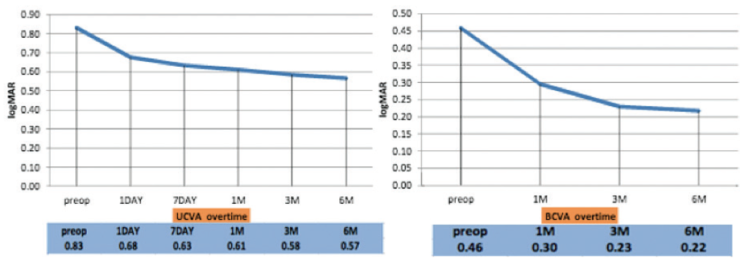
Figure 3. Six-month data from 29 eyes of 29 patients showed improvement in UDVA (left) and CDVA (right) after Keraring SG implantation.
Findings to date also show that Kmax and corneal astigmatism have been reduced and that, overall, patients have gained three Snellen lines of UDVA and CDVA. Additionally, the angle kappa in treated eyes had shifted toward negative values, and negative spherical aberration (C12) had increased as a function of increase in corneal asphericity.
conclusion
These early findings suggest that the Keraring SG has a remodeling effect on the cornea. Further larger, longer-term studies are needed to confirm whether the double-arc ring will lead to stable outcomes. The Keraring SG represents a new design of ICRS that will increase our options for treating patients with corneal ectatic disorders.
1. Gharaibeh AM, Muhsen SM, AbuKhader IB, Ababneh OH, Abu-Ameerh MA, Albdour MD. Keraring intrastromal corneal ring segments for correction of keratoconus. Cornea. 2012; 31(2):115-120.