




Since the introduction of CXL into clinics in the first decade of this century, many changes to the original Dresden protocol have been proposed.1 In particular, new light sources with shorter treatment times due to higher irradiances and new solutions with shorter imbibition times have found their way into clinical routines.2,3 From the surgeon’s point of view, these alterations were significant, as the ratio of treatment time to revenue was low with the Dresden protocol. So far, however, it has mainly been the surgeon—not the patient—who has benefited from these supposed improvements in protocol.
AT A GLANCE
• Customized CXL has a shorter epithelial healing time and a stronger flattening effect than standard CXL, and it provides better regularization of the cornea compared with the standard procedure.
• With further evaluation, refractive CXL might become an option for correction of low myopia in the future.
Three years ago, Avedro introduced the Mosaic System, an adjustable UV-A light source combined with an eye-tracking system. This innovation opened an entirely new field in CXL. Since then, we have been able to project customized irradiation patterns with customized energy profiles onto the cornea.
What is the benefit of treating only parts of the keratoconus cornea instead of the entire cornea? Biomechanical modeling of the crosslinked cornea, performed by Roberts and Dupps, revealed that the entire cornea need not be treated to achieve stabilization of keratoconus; they found that similar results could be obtained if only the weak parts of the keratoconus cornea were stiffened.4
But how do we locate the weakest part of the keratoconus cornea? Measurements of maximal anterior curvature and minimal pachymetry might be erroneous due to compensatory epithelial changes in irregular corneas. Early (unpublished) results of Brillouin microscopy analysis have suggested that, in most cases, maximum posterior float—a parameter measured by several corneal tomography devices—is a good target on which to center an irradiation pattern for keratoconus treatment. (Editor’s Note: For more on Brillouin microscopy, see What is Brillouin Microscopy?)
A NEW TECHNIQUE
At the Institute of Refractive and Ophthalmic Surgery (IROC), we compared customized CXL to standard CXL in eyes with progressive keratoconus.5 We centered customized treatment patterns on the posterior float and used radiant exposure levels of 5 to 10 J/cm². Because the treatment zone is smaller than in standard CXL, we also used a smaller abrasion area for riboflavin imbibition.
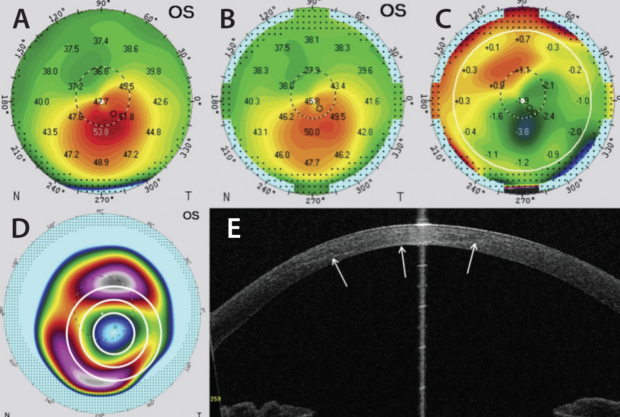
Figure 1. Preoperative axial curvature (A). By 1-year follow-up (B), strong regularization was evident on the difference map (C). Preoperative posterior elevation map with customized CXL treatment pattern overlaid (D). On anterior segment OCT, demarcation line at the 1-month follow-up (white arrows) revealed a Gaussian shape (E).
[Reprinted with permission: Seiler TG, Fischinger I, Koller T, Zapp D, Frueh BE, Seiler T. Customized corneal cross-linking: one-year results. Am J Ophthalmol. 2016;166:14-21.]
Our patients benefited in several ways from the use of this new customized technique. On a short-term basis, due to the smaller abrasion zone, the vulnerable phase during epithelial healing was shortened by almost 1 day. At 1-year follow-up, almost 60% of the eyes showed flattening in maximum keratometry (Kmax) by 1.00 D or more, with significantly higher corneal flattening rates on average.
CASE PRESENTATION
A 27-year-old man was referred to our clinic with documented progressive keratoconus in his left eye (Figure 1A). Complete ophthalmologic examination revealed CDVA of 20/60, and typical keratoconus findings were noted during slit-lamp examination. We performed customized CXL with three concentric circles centered on the posterior float, as shown on the preoperative posterior elevation map (Figure 1D).
Although we used a top-hat profile in every irradiation circle, the demarcation line (Figure 1E, white arrows) at the 1-month follow-up revealed a Gaussian shape. By the 1-year follow-up (Figure 1B), it was obvious that the cornea showed strong regularization (difference map, Figure 1C), with the greatest amount of flattening in the area where the highest energy was applied. In contrast, a compensatory steepening occurred in the formerly flat areas of the cornea.
This observation led us to devise a new regularization index, which consists of the amount in diopters of maximal flattening in the steep areas added to the steepening in diopters in formerly flat areas.
What is Brillouin Microscopy?
By Laura Straub, Editor-in-Chief
Brillouin optical microscopy, a technology developed by Seok Hyun Yun, PhD, and Giuliano Scarcelli, PhD, as a means to monitor corneal stiffness, provides noncontact, real-time in vivo measurement of ocular biomechanical properties.
According to Drs. Yun and Scarcelli, “Brillouin microscopy is based on spectral analysis of light scattered from within corneal tissue. Within the cornea, the interaction between light and microscopic mechanical vibrations that are inherently present thermodynamically causes a small change in the light frequency, so the mechanical information can be measured optically.”
In some of their earliest research, Drs. Yun and Scarcelli measured the age-related stiffening of the crystalline lens in mice in vivo,1 demonstrated mapping of corneal elasticity in both animal and human tissue,2,3 and provided information on the biomechanical effect of keratoconus both ex vivo and in vivo.4,5 They have also used Brillouin microscopy as a quantitative clinical tool for CXL, imaging porcine corneas before and after riboflavin-assisted CXL performed using the Dresden protocol (Figure 1).6
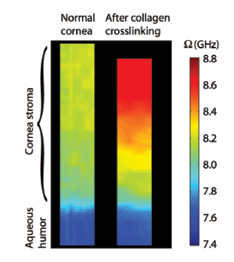
Figure 1. Brillouin images of normal porcine corneal tissue before and after standard epi-off CXL. Imaged area: 800 (z) X 50 μm (x).
Some of the possible uses for Brillouin optical microscopy in CXL and beyond include the following:
• Detection of subtle differences in the biomechanical properties of the cornea, including the amount of stiffening from the anterior to the posterior cornea after CXL and the distribution and magnitude of these changes in three dimensions;
• Early diagnostic tool for keratoconus;
• Assessment of the mechanical outcomes of CXL treatments;
• Preoperative screening tool to search for weak corneas in LASIK candidates; and
• Evaluation of a wide range of ocular features, such as retinochoroidal fluid dynamics and scleral rigidity.
Want to Learn More?
Check out Drs. Scarcelli and Yun’s full article in the archives of CRST Europe.
1. Scarcelli G, Kim P, Yun S. In vivo measurement of age-related stiffening in the crystalline lens by Brillouin optical microscopy. Biophysical J. 2011;101:1539-1545.
2. Scarcelli G, Pineda R, Yun S. Brillouin optical microscopy for corneal biomechanics. Invest Ophthalmol Vis Sci. 2012;53:185-190.
3. Scarcelli G, Yun S. Brillouin optical microscopy of the human eye. Optics Express. 2012;20:9197-9202.
4. Scarcelli G, Besner S, Pineda R, Yun S. Biomechanical characterization of keratoconus corneas ex vivo with Brillouin microscopy. Invest Ophthalmol Vis Sci. 2014;55:4490-4495.
5. Scarcelli G, Besner S, Pineda R, Kalout P, Yun S. In vivo biomechanical mapping of normal and keratoconus corneas. JAMA Ophthalmol.
6. Scarcelli G, Kling S, Quijano E, Pineda R, Marcos S, Yun S. Brillouin microscopy of collagen crosslinking: noncontact depth-dependent analysis of corneal elastic modulus. Invest Ophthalmol Vis Sci. 2013;54:1418-1425.
PERSPECTIVE ON REFRACTIVE CROSSLINKING
When we compare the irradiation pattern with the difference map (Figure 1C), it is obvious that customized CXL created a flattening effect very similar to a myopic correction. This made us curious about the potential use of CXL for myopia correction.
The first preliminary results of CXL used as a refractive procedure are now available. Matthias Elling, MD, of Ruhr University Bochum, presented his group’s first results at the International CXL Experts’ Meeting in Zurich, Switzerland in December.6 The authors attempted low myopia corrections (≤3.00 D), and Dr. Elling reported promising results at 6 months’ follow-up. Longer follow-up times and larger study groups must be evaluated before CXL can be accepted as a refractive procedure.
1. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-A-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620-627.
2. Hammer A, Richoz O, Arba Mosquera S, Tabibian D, Hoogewoud F, Hafezi F. Corneal biomechanical properties at different corneal cross-linking (CXL) irradiances. Invest Ophthalmol Vis Sci. 2014;55:2881-2884.
3. Ehmke T, Seiler TG, Fischinger I, Ripken T, Heisterkamp A, Frueh BE. Comparison of corneal riboflavin gradients using dextran and HPMC solutions. J Refract Surg. 2016;32:798-802.
4. Roberts CJ, Dupps WJ Jr. Biomechanics of corneal ectasia and biomechanical treatments. J Cataract Refract Surg. 2014;40:991-998.
5. Seiler TG, Fischinger I, Koller T, Zapp D, Frueh BE, Seiler T. Customized corneal cross-linking: one-year results. Am J Ophthalmol. 2016;166:14-21.
6. Customized corneal cross-linking for the treatment of myopic refractive error: 6-months results of a prospective clinical study. Paper presented at: International CXL Experts’ Meeting, December 2-3, 2016; Zurich, Switzerland. http://lightforsight.org/wp-content/uploads/sites/5/2016/12/1504-Elling.pptx.pdf. Accessed February 22, 2017.
