



Our group has authored several studies on IOL power calculation after corneal refractive surgery over the past decade.1-9 Thanks to this work, we have also been given the opportunity to write multiple articles on the same subject for CRST Europe.10-12 These papers, as well as the many others written by our colleagues, provide insights into the tools available to calculate IOL power after PRK, LASIK, or RK. However, these articles did not include practical examples in real patients. This article presents four cases that illustrate my approach to IOL power calculation in patients with a history of corneal refractive surgery.
Case No. 1: Previous Myopic PRK With No Preoperative K Readings
A 60-year-old woman had undergone myopic PRK by another surgeon more than 15 years prior to correct -9.00 D in both eyes. She came to our practice in 2016 for cataract surgery, with the goal of bilateral emmetropia. We were unable to retrieve her pre-PRK keratometry (K) readings, so we had to estimate them using the method my colleagues and I recently described.9
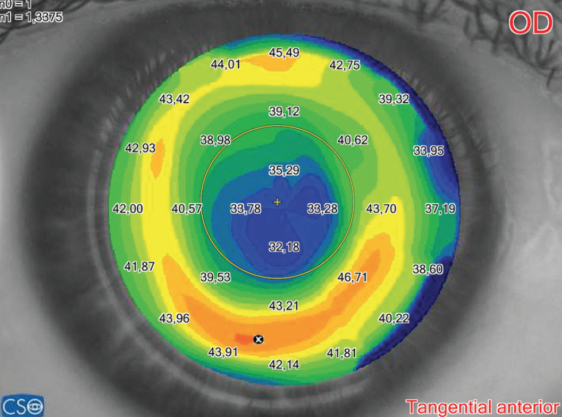
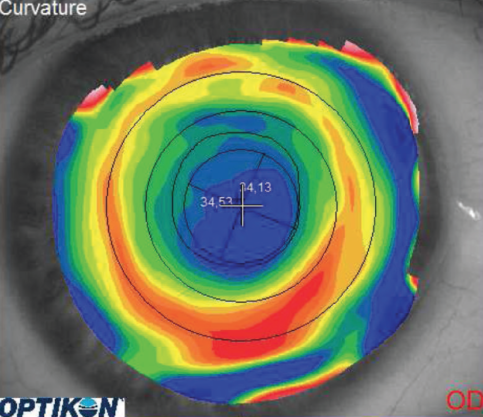
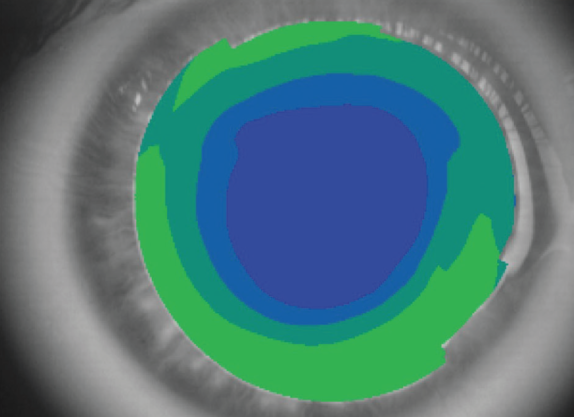
Figure 1. Corneal topography in the right eye of a patient who underwent myopic PRK to correct -9.00 D. The optical zone is large and well centered, reducing the risk of radius error when corneal power must be calculated.
The patient had a posterior corneal radius of 6.91 mm and a posterior Q value of -0.35, as measured by the Pentacam HR (Oculus Optikgeräte). Thus, we were able to estimate a pre-PRK K reading of 40.75 D, which is considerably lower than the average value of 43.81 D reported by Hoffer.13 The estimated 40.75 D preoperative K reading could then be used for IOL calculation methods relying on double-K formulas.14
Multiple corneal topographers showed a relatively large central optical zone, which allowed us to exclude the so-called radius error (Figure 1).15 Optical biometry performed with the Aladdin (Topcon) measured an axial length of 28.59 mm and an anterior chamber depth of 3.67 mm.
Based on the decision tree we published in 2015,8 we utilized the methods of Savini (with double-K SRK/T),2,14 Seitz/Speicher/Savini (with double-K SRK/T),1,14 and Masket.16 Additionally, I always like to test ray tracing, so I also calculated the IOL power with this method using the Sirius (CSO) internal software7 and the Okulix software (Tedics Peric & Jöher) installed on a Galilei G6 (Ziemer). From this device, we also extracted the total corneal power and entered this value into the American Society of Cataract and Refractive Surgery (ASCRS) calculator (http://iolcalc.ascrs.org/).
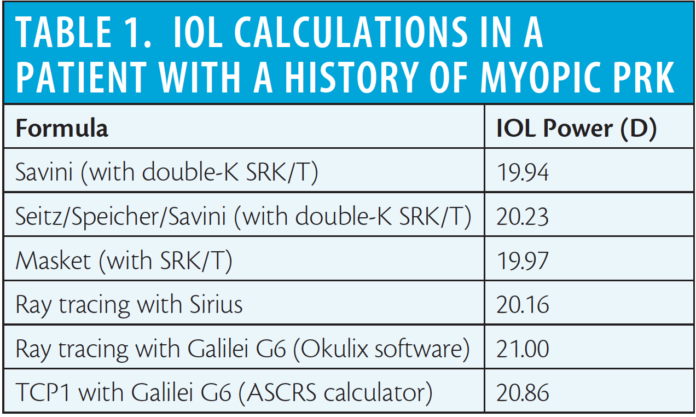
The results of these methods (Table 1) were within 1.06 D of one another. Such a narrow range of results made the choice quite easy, and a 20.50 D IOL power was selected in order to stay within the lowest and highest powers. The patient ended up emmetropic, indicating that all of these methods can be considered reliable.
Case No. 2: Previous Myopic LASIK
In 2006, I performed myopic LASIK on a 51-year-old woman to treat -5.25 -1.25 X 10°. Her mean pre-LASIK K reading was 43.14 D, and her postoperative refraction was plano.
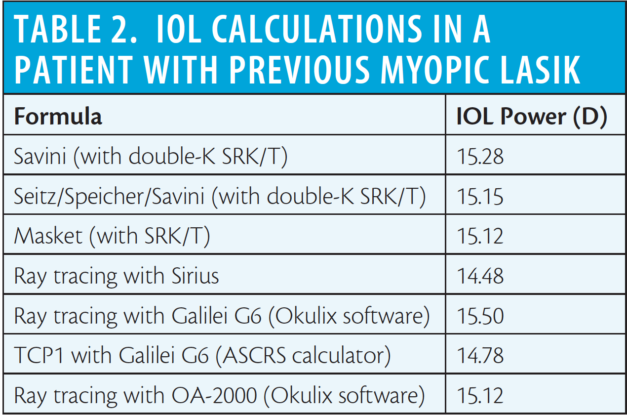
When recently I diagnosed her cataract, corneal topography revealed a large optical zone (Figure 2) with a mean simulated keratometry (sim-K) of 39.06 D. According to optical biometry, the axial length and anterior chamber depth were 28.06 and 3.48 mm, respectively. I followed the aforementioned decision tree and relied on the same methods used in Case No. 1, with the addition of Okulix calculations based on measurements by the OA-2000 optical biometer (Tomey; Table 2).
AT A GLANCE
• Current methods to calculate the IOL power after refractive surgery can lead to accurate results even when preoperative data are unavailable.
• There are only a few methods that can be used to calculate IOL power after RK, most of which have notable limitations.
• Ray tracing does not rely on any fictitious index, such as the keratometric index, and does not require historical data to calculate IOL power.
The IOL power results derived from all but one of the methods in our decision tree ranged from 15.12 to 15.28 D, suggesting that a 15.50 D IOL would be the most logical choice. However, ray tracing with Sirius calculated a lower powered IOL (14.48 D). Therefore, I decided to implant a 15.00 D AcrySof SN60WF (Alcon), and a plano refraction was achieved. Again, this case is useful to confirm that the calculations made by the most accurate methods always produce values in a narrow dioptric range.
Case No. 3: Previous Myopic PRK With NO Preoperative Data
A 55-year-old patient who had previously undergone myopic PRK presented to our clinic, but no preoperative data were available. She did not remember the amount of myopic correction of her PRK, so some methods in the decision tree (Savini and Masket) could not be used. Corneal topography revealed a large and well-centered optical zone (Figure 3). Average sim-K was 41.25 D. Axial length and anterior chamber depth were 25.99 and 3.49 mm, respectively, with the Aladdin. Based on our reported method for calculating preoperative corneal power,9 we estimated a pre-PRK K reading of 43.92 D.
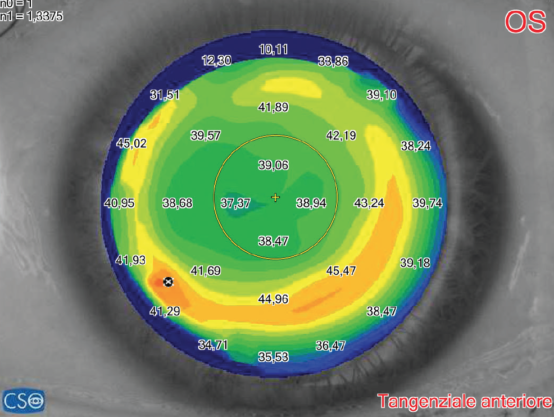
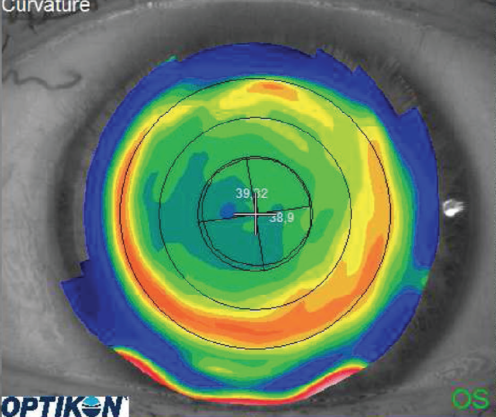
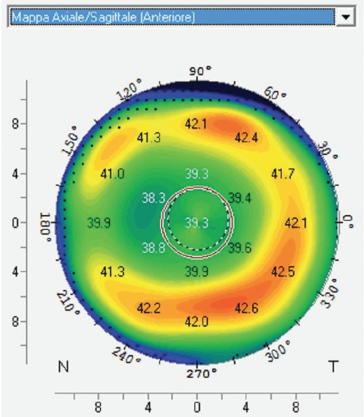
Figure 2. Corneal maps show a large, centered optical zone in the left eye of a patient who had previously undergone LASIK to correct -5.25 -1.25 X 10°.
Our decision tree led us to consider two methods: (1) the Seitz/Speicher/Savini with double-K SRK/T (IOL = 17.24 D) and (2) the Shammas no-history method (IOL = 17.77 D). Additionally, the Barrett True K No History formula (IOL = 17.46 D) could be considered another reliable option. Ray tracing calculated an IOL power of 17.12 D with Sirius and 17.81 D with Galilei and Okulix.
Overall, the range of calculated IOL power was quite narrow (17.12–17.81 D). We chose an IOL power close to the average of these values and implanted a 17.50 D AcrySof SN60WF, which yielded a plano postoperative refraction.
This case confirms that current methods to calculate the IOL power after refractive surgery can lead to accurate results even when preoperative data are unavailable.
Case No. 4: Previous Myopic RK With No Preoperative Data
A 44-year-old man had undergone RK in his right eye 20 years earlier. The patient could not remember if he also underwent subsequent PRK to fine-tune the refraction. His UDVA was 20/200; with a correction of +4.50 +4.50 X 20º, his CDVA was 20/40. Preoperative data were unknown, and the patient’s lens was clear. The corneal map showed a small, centered optical zone, with inferior steepening related to an early peripheral ectasia, which was confirmed by anterior and posterior elevation maps (Figure 4).
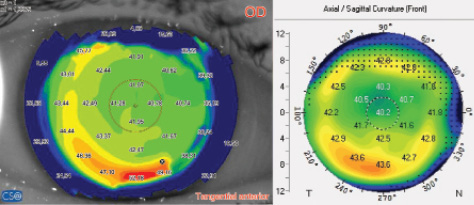
Figure 3. Corneal maps show a large, centered optical zone in the right eye of a patient who had previously undergone myopic PRK. Preoperative data were not available.
I first performed CXL to stabilize the cornea, and, 8 months later, in January 2014, I planned a refractive lens exchange with a toric IOL. The K1 and K2 readings in this eye were 33.32 and 36.04 D. Axial length and anterior chamber depth by immersion ultrasound biometry were 25.47 and 4.34 mm, respectively. Total corneal astigmatism, which should be the target when a toric IOL is used,17 was +3.75 D X 19° with Sirius and +3.70 D X 7° with Pentacam.
Before calculating the IOL power, it is important to note that the sources of error in post-RK eyes are the same as those in post-PRK and post-LASIK eyes. First, the keratometric index (1.3375) is no longer valid because RK disrupts the physiologic anterior-to-posterior corneal curvature ratio. We have shown that RK induces a greater flattening on the posterior corneal surface than on the anterior surface.5 Second, the optical zone is always small, leading to radius error due to the fact that curvature readings are taken outside of the optical zone. Third, the effective lens position is erroneously predicted with theoretical formulas that base this prediction on corneal power.14 Hence, we should not enter unadjusted K readings from any keratometer or topographer and should not use single-K versions of the Holladay 1, Holladay 2, or SRK/T formulas.
There are only a few methods that can be used to calculate IOL power after RK, some of which are included in the ASCRS calculator.18-21 Unfortunately, most of them have notable limitations. For example, they require data that are not always available, such as corneal power by specific corneal topographers such as the Atlas or EyeSys (EyeSys Technologies); they use unadjusted K readings, still based on the keratometric index; in some cases they do not use double-K formulas; and, last, most of them lack formal validation in large samples.
At the time we saw this patient, newer methods, including the Barrett True K and the OCT formula, were not incorporated into the ASCRS calculator, so we could not use them. For these reasons, we relied on ray tracing with Sirius, which predicted a slight myopic spherical equivalent (-0.45 D) with a 32.00 D toric AcrySof SN6AT9. I implanted the lens at an axis of 16°, and the final outcome was a cylinder of +1.00 D X 10°, with a prediction error of -0.95 D.
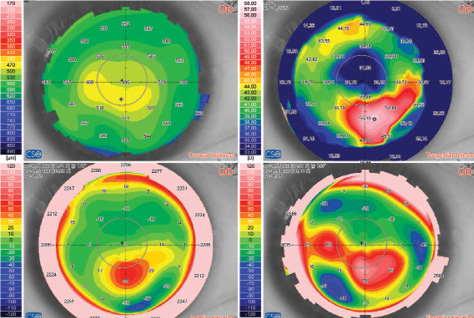
Figure 4. Corneal maps obtained with Scheimpflug imaging show a small central optical zone and inferior steepening with abnormal anterior and posterior elevation in the right eye of a patient with previous RK.
In my experience, this can be considered an excellent result in such a difficult eye. This example demonstrates the advantages of ray tracing, a method that does not rely on any fictitious index, such as the keratometric index, and does not require historical data to calculate IOL power.
CONCLUSION
In eyes with previous corneal refractive surgery, IOL power can be calculated with an accuracy similar to that achieved in unoperated eyes. Ray-tracing software is mandatory to solve the most challenging cases because it is accurate, is easy to use, and does not require historical data. Among classical methods, those included in our published decision tree8 should always be considered.
1. Savini G, Barboni P, Zanini M. Intraocular lens power calculation after myopic refractive surgery. Ophthalmology. 2006;113:1271-1282.
2. Savini G, Barboni P, Zanini M. Correlation between attempted correction and keratometric refractive index of the cornea after myopic excimer laser surgery. J Refract Surg. 2007;23:461-466.
3. Savini G, Barboni P, Profazio V, Zanini M, Hoffer KJ. Corneal power measurements with the Pentacam Scheimpflug camera after myopic excimer laser surgery. J Cataract Refract Surg. 2008;34:809-813.
4. Savini G, Hoffer KJ, Carbonelli M, Barboni P. Intraocular lens power calculation after myopic excimer laser surgery: clinical comparison of published methods. J Cataract Refract Surg. 2010;36:1455-1465.
5. Camellin M, Savini G, Hoffer KJ, Carbonelli M, Barboni P. Scheimpflug camera measurement of anterior and posterior corneal curvature in eyes with previous radial keratotomy. J Refract Surg. 2012;28:275-279.
6. Savini G, Hoffer KJ, Carbonelli M, Barboni P. Scheimpflug analysis of corneal power changes after myopic excimer laser surgery. J Cataract Refract Surg. 2013;39:605-610.
7. Savini G, Bedei A, Barboni P, Ducoli P, Hoffer KJ. Intraocular lens power calculation by ray-tracing after myopic excimer laser surgery. Am J Ophthalmol. 2014;157:150-153.
8. Savini G, Barboni P, Carbonelli M, Ducoli P, Hoffer KJ. Intraocular lens power calculation after myopic excimer laser surgery: selecting the best method using available clinical data. J Cataract Refract Surg. 2015;41:1880-1888.
9. Savini G, Hoffer KJ, Schiano-Lomoriello D, Ducoli P. Estimating the preoperative corneal power with Scheimpflug imaging in eyes that have undergone myopic LASIK. J Refract Surg. 2016;32:332-336.
10. Savini G, Hoffer KJ, Zanini M. IOL power calculation after LASIK and PRK. CRST Europe. April 2007. Available at: http://crstodayeurope.com/articles/2007-apr/0407_09-php/?single=true.
11. Savini G. IOL power calculation after refractive surgery. CRST Europe. May 2015. Available at: http://crstodayeurope.com/articles/2015-may/iol-power-calculation-after-refractive-surgery/.
12. Savini G, Hoffer KJ. As of now. CRST Europe. November/December 2016. Available at: http://crstodayeurope.com/articles/2016-novdec/as-of-now/.
13. Hoffer KJ. Biometry of 7,500 cataractous eyes. Am J Ophthalmol. 1980;90:360-368. Erratum in: Am J Ophthalmol. 1980;90:890.
14. Aramberri J. Intraocular lens power calculation after corneal refractive surgery: double-K method. J Cataract Refract Surg. 2003;29:2063-2068.
15. Savini G, Carbonelli M, Barboni P, Hoffer KJ. Clinical relevance of radius of curvature error in corneal power measurements after excimer laser surgery. J Cataract Refract Surg. 2010;36:82-86.
16. Masket S, Masket SE. Simple regression formula for intraocular lens power adjustment in eyes requiring cataract surgery after excimer laser photoablation. J Cataract Refract Surg. 2006;32:430-434.
17. Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56:827-835.
18. Kim SH, Lee JH. Videokeratography to calculate intraocular lens power after radial keratotomy. J Refract Surg. 2004;20:284-286.
19. Packer M, Brown LK, Hoffman RS, Fine IH. Intraocular lens power calculation after incisional and thermal keratorefractive surgery. J Cataract Refract Surg. 2004;30:1430-1434.
20. Maeda N, Klyce SD, Smolek MK, McDonald MB. Disparity between keratometry-style readings and corneal power within the pupil after refractive surgery for myopia. Cornea. 1997;16:517-24.
21. Awwad ST, Dwarakanathan S, Bowman W, et al. Intraocular lens power calculation after radial keratotomy: estimating the corneal power. J Cataract Refract Surg. 2007;33:1045-1050.
