





Cataract surgery in patients with keratoconus presents multiple challenges. To begin with, the decision of whether to perform surgery is not clear-cut, as it is often difficult to evaluate the cataract’s influence on the patient’s visual acuity. For this reason, surgeons may delay the decision to operate in many cases.
To determine whether cataract extraction will offer substantial visual benefit, a diagnostic contact lens trial with rigid lenses may assist, if the patient does not present with significant scars on the visual axis. This test regularizes irregular astigmatism, showing the real limitation placed on the patient’s vision by other factors such as cataract.
AT A GLANCE
• The distortion of the cornea in keratoconic eyes makes IOL calculation more complex.
• For cataract surgery in keratoconic eyes, the best approach includes proper patient selection, IOL calculation with use of topography and optical biometry, use of a MICS technique, and toric IOL implantation in well-selected cases.
Once the decision to operate is made, IOL calculation and selection is the next challenge. The distortion of the cornea in keratoconic eyes makes IOL calculation more complex. However, the IOL calculation formulas applied are still the same as those used in nonkeratoconic eyes. The measurement of high keratometry (K) values in keratoconic eyes is not always reliable, and results can vary depending on the technology used to calculate the value and where on the cornea the measurement is taken.
TORIC IOL CONSIDERATIONS
Patients with keratoconus may be candidates for toric IOL implantation, which presents a further challenge due to the presence of high amounts of irregular astigmatism associated with corneal toricity. The challenge increases when such eyes have undergone previous corneal surgeries, such as intrastromal corneal ring segment (ICRS) implantation or CXL.
Modern toric IOLs have shown excellent efficacy, predictability, and safety in correcting astigmatism at the time of cataract surgery in eyes with normal corneas and regular astigmatism. Clinical studies have shown significantly better UDVA and refractive astigmatism outcomes after toric IOL implantation compared with spherical IOL implantation in eyes with cylinder powers of 1.50 D or higher. However, there are few published articles on toric IOL performance in keratoconic eyes.1-10
The cornea in a keratoconic eye is multifocal, and the visual axis is not at the apex of the cornea but on the slope of the cone.11 Thus, K readings may be artificially high for the purposes of IOL calculation. It is necessary to remember that the software used in the various toric IOL calculators is calibrated and validated based on data from normal nonkeratoconic eyes with regular astigmatism, in which the apex of the cornea in most cases is almost or totally coincidental with the visual axis.8
Considering this, toric IOL implantation should be used mainly in eyes with mild to moderate nonprogressive keratoconus with adequately regular astigmatism in the central 4 mm of the cornea.2,8-10
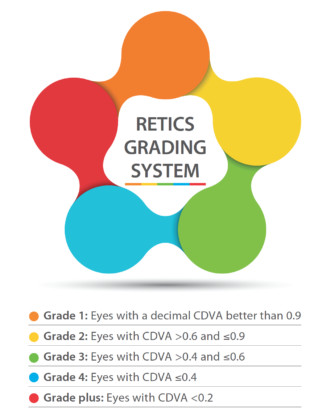
GRADING SYSTEM
Our research group has devised a keratoconus grading system called Redes Temáticas de Investigación Cooperativa en Salud (RETICS; Thematic Networks of Cooperative Research in Health). This classification is mainly based on CDVA but also includes some aberrometric parameters such as root-mean-square, coma-like, internal astigmatism, and asphericity.12
The RETICS grading system provides functional classification of visual acuity. According to this system, illustrated above, cataract surgery with toric IOL implantation can be performed in grade 1 eyes and selected grade 2 eyes (Figures 1 and 2). For eyes with other grades, a corneal reshaping procedure such as ICRS implantation should be attempted before cataract surgery.
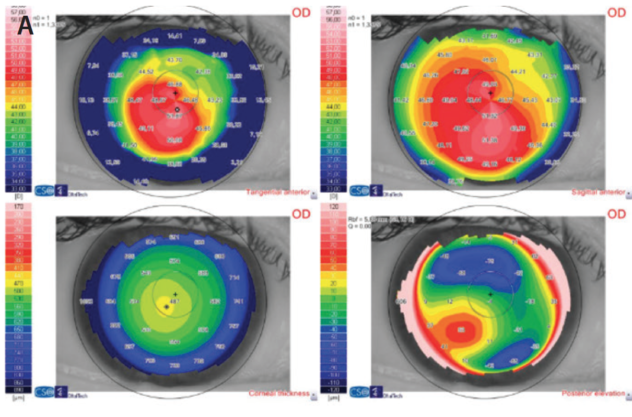
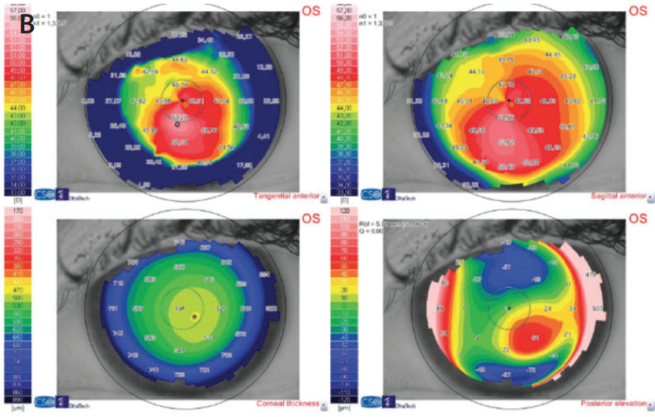
Figure 1. Topography maps of the right (A) and left (B) eyes of a patient with bilateral moderate stable keratoconus. The right eye refraction is -4.50 -4.00 X 45º with a historical CDVA of 0.98 (decimal scale). The left eye refraction is -4.25 -3.00 X 155º with a historical CDVA of 1.0. According to the RETICS grading system, this patient is a good candidate for cataract surgery with toric IOL implantation.
IOL CALCULATION IN THE KERATOCONIC EYE
The SRK II formula has been used for IOL power calculation in patients with keratoconus.9 Some surgeons choose K values obtained with the Pentacam (Oculus Optikgeräte) for IOL calculation; however, for these eyes, manual keratometry (Javal-Schiotz) may be used to obtain accurate determination of the axis of corneal astigmatism, and the SRK/T may be the preferred formula.2
In the largest series of refractive lens exchange in patients with keratoconus,13 IOL power was calculated using ultrasound biometry with the Humphrey 820 (Allergan) and the Holladay 2 formula, targeting residual myopic astigmatism. K readings were obtained using axial topographic maps. The dioptric power of the steepest meridian over the central 3 mm of the cornea was considered K2, and the dioptric power of the flattest meridian over the central 3 mm of the cornea was considered K1. Each meridian power was calculated by averaging its two semi-meridian values, always considering the central 3 mm.13
In a series of two eyes with forme frustre keratoconus, IOL calculation was performed using axial length measured by IOLMaster (Carl Zeiss Meditec), K readings from the Orbscan II (Bausch + Lomb), and the SRK II formula.8,14
Clearly, there is disparity among authors regarding the best method for IOL calculation in patients with keratoconus. In any case, the preferred measurement instruments are optical interferometry for axial length measurement and corneal topography for K readings.
In our own study,10 we had the impression that, when corneal shape is greatly altered, the deformity of the anterior and posterior cornea is likely similar; therefore, the posterior cornea may not influence IOL calculation as much as was previously thought.
Figure 2. A patient with cataract and steep keratoconus with contact lens intolerance. The right eye refraction is -1.00 -2.00 X 40º (CDVA: 0.4). In this case and in using the RETICS grading system, ICRS implantation to improve corneal regularity and decrease the coma aberration, followed by cataract surgery with toric IOL implantation, was recommended.
In this case series, the SRK/T formula seemed to provide better results than the Hoffer Q.10 By contrast, another group of authors analyzed the difference between the ideal and the calculated IOL power with the SRK, SRK II, and SRK/T formulas, and the most accurate IOL power was found with the SRK II.1
Formulas that take into consideration axial length and other factors that help to predict effective lens position (ELP), such as the Holladay 2, should be more accurate. It is hoped that new ray-tracing formulas that assess total corneal power, taking into account posterior corneal surface astigmatism, will help us to improve predictability in these difficult eyes even more in the future. However, recent studies have not demonstrated better outcomes using these formulas in nonkeratoconic eyes.15,16 Larger series are needed to help elucidate which formula performs best.
LENS SURGERY IN KERATOCONIC EYES
It is extremely important to avoid surgically induced astigmatism (SIA) in keratoconic eyes. Microincision cataract surgery (MICS) may be the preferred approach in these eyes, as incisions larger than 2.2 mm may induce variable amounts of SIA, leading to more unpredictable outcomes.17-19 Other factors that can affect SIA are preoperative corneal astigmatism, suture use, and patient age.20,21
Our research group recently published the results of MICS in a series of keratoconic eyes.10 Surprisingly, in most papers published to date, the incisions used to perform surgery have been larger than 2.2 mm, and only two studies used an incision size of 2.2 mm or smaller.2,10 Other authors have reported use of 2.7- and 3.2-mm scleral tunnel incisions8,12 and 2.8- and 3.2-mm corneal incisions.9,14 However, it is important to emphasize that large corneal incisions must be avoided in keratoconus due to their weakening effect in these already-weak corneas. The smaller the corneal incision, the better.
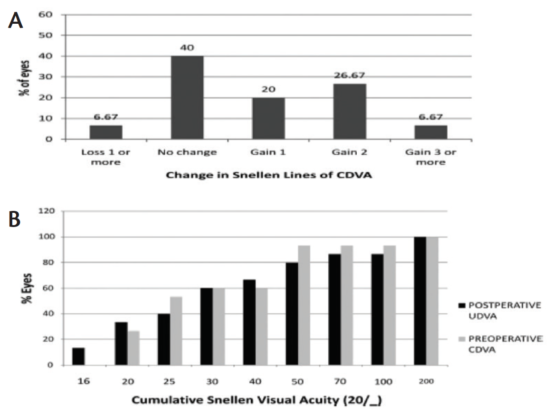
Figure 3. The change in Snellen lines of CDVA versus percentage of eyes (A) and the results for visual efficacy (B).
Some manufacturers’ toric IOL calculators consider the relation between cylinder power at the IOL plane and at the corneal plane as a fixed value.22,23 This is a significant error because the effective cylinder power of the IOL at the corneal plane is a function of the ELP and the spheroequivalent power of the IOL. The IOL cylindrical and spherical powers must first be converted into the two principal lens powers, after which both lens powers are calculated to the corneal plane using a standard vertex formula. The difference between both lens powers at the corneal plane should be used to select the most appropriate IOL cylinder power.3
Results. Cataract surgery with toric IOL implantation in patients with keratoconus can yield good outcomes. Nanavaty et al8 reported excellent results, with postoperative UDVA of 20/40 or better in 75% of eyes and reduction in cylinder from 3.00 ±1.00 D preoperatively to 0.70 ±0.80 D.
Leccisotti13 reported worse outcomes in his series of clear lens extraction and toric IOL implantation: IOL exchange surgery was needed in 11 cases (32%) because the IOL power was not accurate due to the limitations of ultrasound biometry. At 12 months, mean spherical equivalent (SE) was -1.31 ±1.08 D, and mean defocus equivalent was 1.94 ±1.57 D. Further, 22 eyes (65%) were within ±2.00 D of defocus equivalent, 16 (47%) within ±1.00 D, and three (9%) within ±0.50 D. The safety index was 1.38, and the efficacy index was 0.87.
In a series of 19 keratoconic eyes undergoing refractive lens exchange, Jaimes et al9 reported that mean sphere decreased from -5.25 ±6.40 D preoperatively to 0.22 ±1.01 D postoperatively (P<.001). Mean preoperative cylinder and SE were 3.95 ±1.30 and -7.10 ±6.42 D, respectively, improving to 1.36 ±1.17 and -0.46 ±1.12 D after surgery (P<.001). Mean UDVA was 1.35 ±0.36 D preoperatively and 0.29 ±0.23 D after surgery (P<.001).
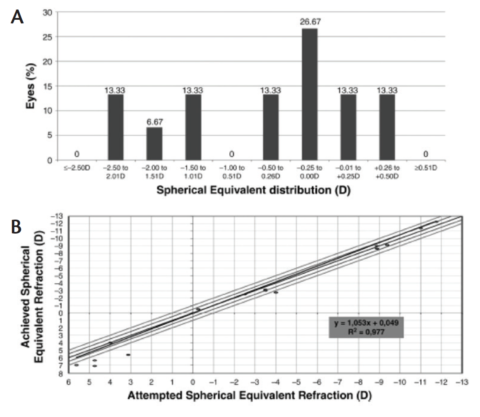
Figure 4. The postoperative spherical equivalent distribution (A) and attempted versus achieved refraction (B). In B, the black line corresponds to the fit line of the complete group.
Thepatiphat et al1 reported a mean improvement in CDVA of 4 lines and a slight improvement in UDVA from 0.71 ±0.41 to 0.63 ±0.47 D; most of these patients were rigid contact lens wearers both before and after surgery.
Our research group recently published the largest series of MICS with toric IOL implantation in keratoconic eyes (n=17).10 Statistically significant improvements from pre- to postoperative were seen in cylinder, defocus equivalent, UDVA, and CDVA. Keratometry remained stable due to the neutral effect of the MICS incisions. Nine eyes (60%) achieved a postoperative UDVA of 20/30 or better. The efficacy and safety indexes were 1.17 ±0.66 and 1.38 ±0.58, respectively. Figure 3 shows the change in Snellen lines of CDVA versus percentage of eyes and the visual efficacy results. In Figure 4, the postoperative SE distribution and the attempted versus achieved refraction are shown. The black line corresponds to the fit line of the complete group.
According to the literature reviewed above, toric IOL implantation at the time of cataract surgery in keratoconic eyes can reduce preoperative cylinder and improve refraction. However, the predictability achieved is worse than and not comparable with the predictability reported in eyes with normal corneas.3,4,24-34
CONCLUSION
Cataract surgery in keratoconic eyes can improve patients’ refraction and quality of life. To achieve a satisfactory outcome, proper patient selection, IOL calculation with use of topography and optical biometry, use of a MICS technique, and toric IOL implantation in well-selected cases comprise the best approach. Eyes with posterior keratoconus present additional unique challenges.33
1. Thebpatiphat N, Hammersmith KM, Rapuano CJ, et al. Cataract surgery in keratoconus. Eye Contact Lens. 2007;33:244-246.
2. Visser N, Gast ST, Bauer NJ, et al. Cataract surgery with toric intraocular lens implantation in keratoconus: a case report. Cornea. 2011;30:720-723.
3. Visser N, Bauer N, Nuijts R. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes and complications. J Cataract Refract Surg. 2013;39:624-637.
4. Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller KM. The AcrySof toric intraocular lens in subjects with cataracts and corneal astigmatism; a randomized, subject-masked, parallel group, 1-year study. Ophthalmology. 2010;117:2104-2111.
5. Statham M, Apel A, Stephensen D. Comparison of the AcrySof SA60 spherical intraocular lens and the AcrySof Toric SN60T3 intraocular lens outcomes in patients with low amounts of corneal astigmatism. Clin Exp Ophthalmol. 2009;37:775-779.
6. Ernest P, Potvin R. Effects of preoperative corneal astigmatism orientation on results with a low-cylinder-power toric intraocular lens. J Cataract Refract Surg. 2011;37:727-732.
7. Lee SJ, Kwon HS, Koh IH. Sequential intrastromal corneal ring implantation and cataract surgery in a severe keratoconus patient with cataract. Korean J Ophthalmol. 2012;26:226-229.
8. Nanavaty MA, Lake DB, Daya SM. Outcomes of pseudophakic toric intraocular lens implantation in keratoconic eyes with cataract. J Refract Surg. 2012;28:884-889.
9. Jaimes M, Xacur-Garcia F, Alvarez-Melloni D, et al. Refractive lens exchange with toric intraocular lenses in keratoconus. J Refract Surg. 2011;27:658-664.
10. Alió JL, Peña-García P, Abdulla Guliyeva F, Soria FA, Zein G, Abu-Mustafa SK. MICS with toric intraocular lenses in keratoconus: outcomes and predictability analysis of postoperative refraction. Br J Opthalmol. 2014;98(3):365-370.
11. Tan B, Baker K, Chen YL, et al. How keratoconus influences optical performance of the eye. J Vis. 2008;8(2):13.1-10.
12. Vega-Estrada A, Alio JL, Brenner LF, et al. Outcome analysis of intracorneal ring segments for the treatment of keratoconus based on visual, refractive, and aberrometric impairment. Am J Ophthalmol. 2013;155:575-584.
13. Leccisotti A. Refractive lens exchange in keratoconus. J Cataract Refract Surg. 2006;32:742-746.
14. Navas A, Suárez R. One-year follow-up of toric intraocular lens implantation in forme fruste keratoconus. J Cataract Refract Surg. 2009;35:2024-2027.
15. Zhang L, Sy ME, Mai H, et al. Effect of posterior corneal astigmatism on refractive outcomes after toric intraocular lens implantation. J Cataract Refract Surg. 2015;41:84-89.
16. Reitblat O, Levy A, Kleinmann G, et al. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: Comparison of methodologies. J Cataract Refract Surg. 2016;42(2):217-225.
17. Kohnen T, Dick B, Jacobi KW. Comparison of the induced astigmatism after temporal clear corneal tunnel incisions of different sizes. J Cataract Refract Surg. 1995;21:417-424.
18. Oshika T, Nagahara K, Yaguchi S, et al. Three year prospective, randomized evaluation of intraocular lens implantation through 3.2 and 5.5 mm incisions. J Cataract Refract Surg. 1998;24:509-514.
19. Masket S, Wang L, Belani S. Induced astigmatism with 2.2- and 3.0-mm coaxial phacoemulsification incisions. J Refract Surg. 2009;25:21-24.
20. Lyhne N, Corydon L. Two year follow-up of astigmatism after phacoemulsification with adjusted and unadjusted sutured versus sutureless 5.2 mm superior scleral incisions. J Cataract Refract Surg. 1998;24:1647-1651.
21. Storr-Paulsen A, Madsen H, Perriard A. Possible factors modifying the surgically induced astigmatism in cataract surgery. Acta Ophthalmol Scand. 1999;77:548-551.
22. Goggin M, Moore S, Esterman A. Outcome of toric intraocular lens implantation after adjusting for anterior chamber depth and intraocular lens sphere equivalent power effects. Arch Ophthalmol. 2011;129:998-1003.
23. Holladay JT. Exact toric intraocular lens calculations using currently available lens constants [letter]. Arch Ophthalmol. 2012;130:946-947.
24. Kim MH, Chung T-Y, Chung E-S. Long-term efficacy and rotational stability of AcrySof toric intraocular lens implantation in cataract surgery. Korean J Ophthalmol. 2010;24:207-212.
25. Mingo D, Muñoz-Negrete FJ, Kim HRW, Morcillo R, Rebolleda G, Oblanca N. Comparison of toric intraocular lenses and peripheral corneal relaxing incisions to treat astigmatism during cataract surgery. J Cataract Refract Surg. 2010;36:1700-1708.
26. Cervantes G, Garcia L, Mendoza E, Velasco C. High-cylinder acrylic toric intraocular lenses: a case series of eyes with cataracts and large amounts of corneal astigmatism. J Refract Surg. 2012;28:302-304.
27. Alió JL, Piñero DP, Tomás J, Alesón A. Vector analysis of astigmatic changes after cataract surgery with toric intraocular lens implantation. J Cataract Refract Surg. 2011;37:1038-1049.
28. Tassignon MJ, Gobin L, Mathysen D, Van Looveren J. Clinical results after spherotoric intraocular lens implantation using the bag-in-the-lens technique. J Cataract Refract Surg. 2011;37:830-834.
29. Alió JL, Agdeppa MCC, Pongo VC, El Kady B. Microincision cataract surgery with toric intraocular lens implantation for correcting moderate and high astigmatism: pilot study. J Cataract Refract Surg. 2010;36:44-52.
30. Ahmed IIK, Rocha G, Slomovic AR, Climenhaga H, Gohill J, Grégoire A, Ma J; Canadian Toric Study Group. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cataract Refract Surg. 2010;36:609-616.
31. Ernest P, Potvin R. Effects of preoperative corneal astigmatism orientation on results with a low-cylinder-power toric intraocular lens. J Cataract Refract Surg. 2011;37:727-732.
32. Wade M, Steinert RF, Garg S, Farid M, Gaster R. Results of toric intraocular lenses for post-penetrating keratoplasty astigmatism. Ophthalmology. 2014;121:771-777.
33. Bozorg S, Pineda R. Cataract and keratoconus: minimizing complications in intraocular lens calculations. Semin Ophthalmol. 2014;29(5-6):376-9. Review.
34. Tamaoki A, Kojima T, Hasegawa A, Nakamura H, Tanaka K, Ichikawa K Intraocular lens power calculation in cases with posterior keratoconus. J Cataract Refract Surg. 2015;41(10):2190-2195.
