



Incisions play an important role throughout the entire cataract surgery procedure, from the first steps to the postoperative period. Proper incision architecture and wound configuration are crucial for, among other things, prophylaxis of endophthalmitis—one of the most dreaded complications of cataract surgery.
This article details five fundamental concepts for creating the perfect wound.

SCLERAL AND CORNEAL INCISIONS EACH HAVE POSITIVE FEATURES
Surgeon preference for clear corneal incisions (CCIs) over scleral incisions has grown in the past decade; however, many studies—particularly those conducted after 2000—suggest that there is a greater risk of endophthalmitis with the adoption of CCIs.1 Therefore, the methods used to create these incisions are key.
AT A GLANCE
- Well-configured and well-constructed incisions facilitate all steps of cataract surgery.
- Risk of endophthalmitis, the most feared complication of cataract surgery, is closely related to incision quality.
- Understanding good wound configuration for main and sideport incisions helps to attain better fluidics during surgery and facilitates postoperative healing.
Scleral incisions are more astigmatically neutral than corneal incisions. They rarely leak because the tissue bed is vascularized and more elastic than corneal tissue, enabling the use of larger incision sizes. Scleral incisions are particularly useful for nonemulsifiable rock-hard cataracts and rigid IOL implantation. However, risk of conjunctival trauma arises from the use of more instruments and cautery when scleral incisions are performed.

THE ADVANTAGES OF SUPERIOR AND TEMPORAL INCISIONS DIFFER
Temporal incisions allow better visualization of intraocular structures during surgery than superior incisions. Longer tunnels are possible, and incisions yield less risk of bleeding and conjunctival ballooning when located temporally. Moreover, temporal incisions are easier to create in patients with protruding eyebrows.
On the other hand, because the cornea is oval, superior incisions are closer to the center of the eye than temporal incisions. Further, the superior eyelid may protect superior wounds in patients who rub their eyes.
Astigmatic changes. The incisional funnel is an imaginary pair of lines, beginning approximately 3 mm apart and diverging from the limbus (Figure 1). Incisions made within this funnel will be astigmatically neutral, and incisions made anteriorly will result in more postoperative astigmatism than those made posteriorly.

Figure 1. The incisional funnel is an imaginary pair of lines, approximately 3 mm apart and diverging from the limbus. Incisions made within this funnel will be astigmatically neutral.
Again, because the cornea is oval, temporal incisions are created further away from the center of the eye, and therefore they induce less astigmatism. Although studies have shown that temporal incisions tend to induce less astigmatism compared with superior incisions,2,3 it should be noted that some older studies were done with larger incisions than are commonly used today; the difference in astigmatic changes between superior and temporal incisions is less pronounced in more recent studies.3

BLADE MATERIAL AND DESIGN ARE IMPORTANT VARIABLES
Blade material. The quality of an incision can be assessed by the need for less stromal hydration, which is an indicator of a high-quality blade.
A sharper blade allows incisions to be created with reduced trauma and increased control compared with duller blades. The harder the material, the sharper the blade, and the hardest material available is diamond (Figure 2). The use of a sharp diamond blade, however, may also increase the risk of catching the capsule, so diamond knives are usually not suitable for trainees. They are also costly to purchase and repair and require special handling.
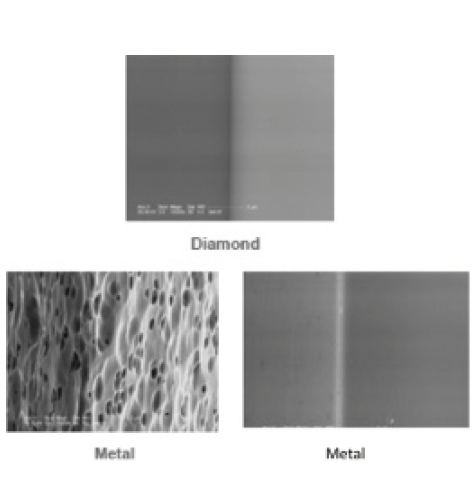
Figure 2. Diamond blades are sharpest; the quality and consistency of metal blades varies widely.
Metal blades can be made of flattened wire or flat stock steel. These blades undergo multiple manufacturing steps, including grinding, honing, coining, and electrochemical polishing. Thus, significant variation in the quality and consistency of metal blades may be seen from one manufacturer to another (Figure 2).
Blade design. Keratomes should be designed with minimal front-end resistance, such as with a beveled front end, to allow easy tissue penetration. The resistance should increase gradually with tissue passage to allow more control. Blade designs without a sharp shoulder can help to prevent inadvertent damage to intraocular structures such as the capsule and iris.

PROPER WOUND CONFIGURATION IS KEY
Wound shape. It has been clearly shown that a wound that is nearly square is more stable and may induce less astigmatism than a rectangular wound.4
Wound size. Short CCIs may tend to leak and require extra stromal hydration or suturing. They may also be associated with iris prolapse. With long clear corneal tunnel incisions, corneal striae are common, the surgeon has less maneuverability, and there is a higher likelihood of wound burn. A CCI with a chord length of least of 2 mm is adequate to achieve self-sealing.5
Do not over-fill the anterior chamber with OVD. When this is done, the likelihood of creating a shorter and straighter tunnel than intended is increased.
Stab versus multiplanar incision. Studies using anterior segment OCT have shown endothelial gaping and loss of coaptation (Figure 3) after the creation of CCIs; this suggests that these incisions may still be weak after epithelial healing and are likely to open transiently with little force, particularly in patients with low postoperative IOP.6-9 Endothelial gaping and loss of coaptation are greater when postoperative IOP is low, and this is a major cause of anterior chamber contamination. Therefore, the surgeon should ensure that IOP is within normal range at the end of surgery.9
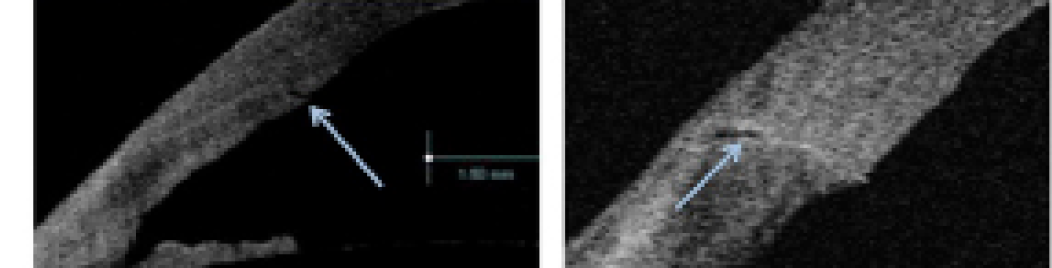
Figure 3. Studies using anterior segment OCT have shown endothelial gaping and loss of wound coaptation. [Reprinted with permission from Calladine D, Packard R. Clear corneal incision architecture in the immediate postoperative period evaluated using optical coherence tomography. J Cataract Refract Surg. 2007;33:1429-1435.]
In 1862, the famed microbiologist Louis Pasteur demonstrated that multiplanar entrances have advantages over straight entrances in his experiment to disprove the existence of spontaneous generation. Pasteur grew microorganisms in two bottles, one with a straight opening and the other with a curved opening. He then boiled both bottles to sterilize them. He found that the bottle with the curved opening remained sterile over time, but new organisms developed in the straight bottle (Figure 4).
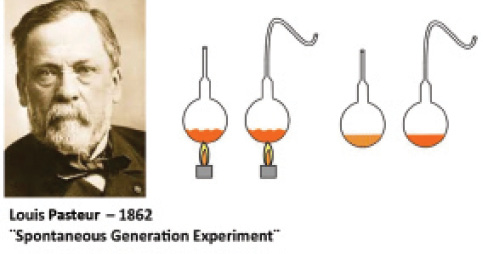
Figure 4. Louis Pasteur sterilized two bottles, one with a straight opening and the other with a curved opening. The bottle with the curved opening remained sterile over time, while microorganisms grew in the bottle with the straight opening.
As suggested by this experiment, proper wound construction is important to prevent or minimize the contamination of the aqueous humor from the environment outside the eye—a frequent source of the infectious agents that cause endophthalmitis. At low IOP levels, the vertical walls of an incision may collapse and prevent wound seal, whereas, at high IOP levels, the horizontal walls stick together and promote wound seal (Figure 5).7
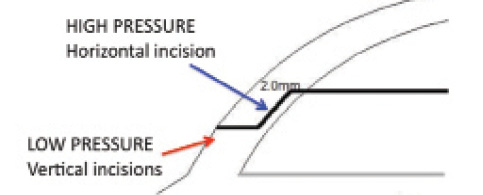
Figure 5. At low IOP levels, the vertical walls of an incision may collapse and prevent wound seal. At high IOP levels, the horizontal walls stick together and secure the wound.
Wound stretch. The surgeon should aim to minimize maneuvers that may stretch the incision. Caution should be exercised when implanting IOLs of high powers, particularly when using a wound-assisted IOL insertion technique in which the incision is used as a forward extension of the cartridge tip.
Wound burn. Risk factors for wound burn include hard cataracts, interruption of irrigation and aspiration during nucleus occlusion, clogging of the phaco tip, and tight and long incisions (Figure 6). If any of these scenarios are encountered, phaco and fluidics settings should be adjusted to ensure minimal occlusion and use of phaco power. Cooling with frequent irrigation of the wound during surgery may also be helpful.

Figure 6. Risk factors for wound burn include hard cataracts, interruption of irrigation and aspiration during occlusion, clogging of the phaco tip, and tight and long incisions.
If wound burn occurs, the incision should be closed with multiple interrupted sutures, and the patient should be closely followed. Wound burn can induce significant astigmatism, which commonly returns to normal within 3 months after surgery.
Stromal hydration and Descemet membrane detachment. Anterior segment OCT studies have shown that local Descemet membrane detachment and misalignment are fairly common after stromal hydration.8,9 Most CCIs, whether hydrated or not, appear to seal immediately after surgery and demonstrate no leakage on Seidel testing. Therefore, surgeons should take care not to overhydrate and increase the risk of damaging Descemet membrane.
Sutures. Sutures are the standard way to seal corneal incisions because of their efficiency and strength. The tautness of the sutures should be adjusted so that they do not allow fluid influx when stress is placed on certain areas.

SIDEPORT INCISIONS SHOULD BE FITTED TO THE SIZE OF THE SECOND INSTRUMENT
To minimize chamber fluctuation during surgery, sideport incisions should be designed to fit the diameter of the surgeon’s second instrument. If the incision is larger than the instrument, there may be leakage during surgery, and nuclear pieces may not come to the phaco tip. Additionally, leakage can bring the posterior capsule closer to the tip during phacoemulsification and irrigation and aspiration. On the other hand, if the sideport incisions are too tight, corneal striae may result, obscuring the surgeon’s vision.
Sideport incisions tend to leak more than central incisions because they are subjected to more stretching, particularly in bimanual microincisional surgery. Therefore, sideport incisions should be carefully checked for leaks at the end of the surgery to minimize the risk of infection, IOP fluctuation, and instability of IOL positioning.
CONCLUSION
CCIs are preferred over scleral tunnels, but scleral tunnels may be the optimal choice in eyes with rock-hard cataracts or when a rigid lens is to be implanted. Temporal incisions are typically preferred today over superior incisions, mainly because of better intraocular visibility during surgery and less induction of astigmatism.
Diamond blades create the best quality cuts, but beginning surgeons should take care when using these instruments. There is variability among metal blades, so the surgeon should be aware of the quality of the metal blade he or she is using.
To minimize leakage and promote the best wound seal, multiplanar or curved incisions are preferable over stab incisions. Finally, optimal wound healing occurs when good wound construction is carried out.
1. Taban M, Behrens A, Newcomb RL, et al. Incidence of acute endophthalmitis following cataract surgery: a systematic review. Arch Ophthalmol. 2005;123:613-620.
2. Simsek S, Yasar T, Demirok A, Cinal A, Yilmaz OF. Effect of superior and temporal clear corneal incisions on astigmatism after sutureless phacoemulsification. J Cataract Refract Surg. 1998;24:515-518.
3. Can I, Takmaz T, Yıldız Y, Bayhan HA, Soyugelen G, Bostancı B. Coaxial, microcoaxial, and biaxial microincision cataract surgery prospective comparative study. J Cataract Refract Surg. 2010;36:740-746.
4. Ernest PH, Lavery KT, and Kiessling LA. Relative strength of scleral corneal and clear corneal incisions constructed in cadaver eyes. J Cataract Refract Surg. 1994;20:626-629.
5. Fine IH, Hoffman RS, Packer M. Profile of clear corneal incisions demonstrated by ocular coherence tomography. J Cataract Refract Surg. 2007;33:94-97.
6. Chawdhary S, Anand A. Early post-phacoemulsification hypotony as a risk factor for intraocular contamination: in vivo model. J Cataract Refract Surg. 2006;32:609-613.
7. May W, Castro-Combs J, Camacho W, Wittmann P, Behrens A. Analysis of clear corneal incision integrity in an ex vivo model. J Cataract Refract Surg. 2008;34:1013-1018.
8. Hayashi K, Yoshida M, Manabe S, Yoshimura K. Effect of high pressurization versus normal pressurization on changes in intraocular pressure immediately after clear corneal cataract surgery. J Cataract Refract Surg. 2014;40:84-97.
9. Calladine D, Packard R. Clear corneal incision architecture in the immediate postoperative period evaluated using optical coherence tomography. J Cataract Refract Surg. 2007;33:1429-1435.