



Endoscopic cyclophotocoagulation (ECP; Figure 1) has been used in the treatment of glaucoma for more than 20 years. There has been such a bright spotlight on the recent tsunami in new microinvasive glaucoma surgery (MIGS) procedures that it is easy to forget this older MIGS tool that has long been at our disposal. Despite many new entries in the market, ECP remains an attractive option as a standalone or combined procedure and is appropriate for a variety of glaucoma patients.
AT A GLANCE
- ECP can precisely treat the ciliary processes to shrink and efface them without gross architectural destruction or collateral damage.
- When ECP is combined with phacoemulsification, it is usually possible for the patient to discontinue one or two glaucoma medications.
- The procedure can also be combined with other MIGS outflow procedures to increase IOP-lowering, or it can be performed after glaucoma drainage procedures in patients with refractory glaucoma.
In ECP, the combination of diode laser cyclophotocoagulation with an endoscope creates an ab interno procedure that can precisely treat the ciliary processes (Figure 2), shrinking and effacing them without gross architectural destruction or collateral damage. The result is effective reduction of aqueous humor production and secretion. A review of published ECP studies by Kaplowitz and colleagues found reports of IOP reduction ranging from 18% to 47%.1 Although there is more data on the use of ECP in refractory glaucoma, several studies also demonstrate its efficacy and safety as a primary treatment.1

Figure 1. ECP is an aqueous inflow–reducing procedure.

Figure 2. Endoscopic image of treated ciliary processes.
My own experience with the EndoOptiks E2 laser and endoscope system (Beaver-Visitec International) suggests that, when ECP is combined with phacoemulsification (Figure 3), it is usually possible for the patient to discontinue one or two glaucoma medications. This is an excellent option for angle-closure glaucoma patients in particular.
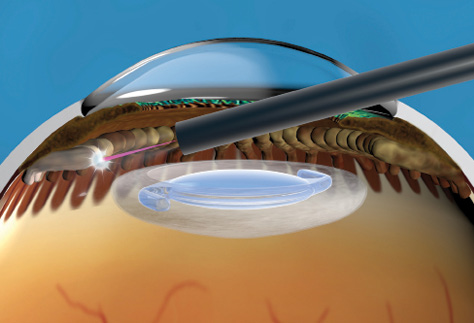
Figure 3. Treatment of the ciliary processes following phacoemulsification.
My own experience with the EndoOptiks E2 laser and endoscope system (Beaver-Visitec International) suggests that, when ECP is combined with phacoemulsification (Figure 3), it is usually possible for the patient to discontinue one or two glaucoma medications. This is an excellent option for angle-closure glaucoma patients in particular.
OPTION TO COMBINE WITH AN OUTFLOW PROCEDURE
ECP is one of the few procedures that works on the aqueous inflow mechanism rather than the outflow pathways. Therefore, ECP can be combined with an outflow procedure, following the same line of thinking we use in combining the common pharmacologic treatment regimen of a prostaglandin with a beta-blocker.
Most MIGS procedures have only recent US FDA approval, and the data available on their safety and efficacy are limited. One approach that has been recently investigated is a combination of the iStent Trabecular Micro Bypass (Glaukos) device, cataract surgery, and ECP, a procedure known as ICE.2 In a series of 70 patients with moderate glaucoma who underwent this ICE triple procedure, the safety profile of cataract surgery alone was maintained and IOP and medication usage were reduced in the majority of patients.2
MAXIMIZING ECP EFFICACY
The following three tips can help to ensure obtaining the best results with ECP.
Tip No. 1: Treat thoroughly. I have noticed that most surgeons tend to under-treat with ECP, which causes them to have to re-treat. The full 360° should be treated, including the entire ciliary processes and the areas between each process, with the goal of applying laser to as much of the ciliary epithelium as possible. This is best done with a curved probe, treating first via the main temporal cataract incision and then via the paracentesis. The surgeon should not be concerned that this will result in excessive lowering of IOP, as the entire ciliary epithelium cannot be reached via an anterior approach. With the posterior aspect spared, the risk of hypotony is eliminated.
Tip No. 2: Start conservatively. Having just said treat thoroughly, let me add that one must start conservatively until full comfort with the 2-D image provided by the endoscope is obtained. If necessary, there is always the option to go back and re-treat. With this strategy, success should increase as one gains experience and facility with the endoscope.
Tip No. 3: Plan for inflammation. ECP causes more inflammation than phacoemulsification alone, and this is best combated prophylactically. Intracameral injection of a steroid at the end of the procedure is ideal, and I also generally prescribe frequent postoperative topical steroids and NSAIDs.
CONCLUSION
ECP is the original MIGS procedure. When it is combined with cataract surgery, the laser probe can be inserted through the main cataract incision or a paracentesis, requiring no additional incision creation or expansion. The procedure is fast, sutureless, and does not damage the ocular surface. It can be combined with cataract surgery in patients with mild to moderate glaucoma, it can be combined with other MIGS outflow procedures to increase IOP-lowering, and it can be performed after glaucoma drainage procedures in patients with refractory glaucoma. This unparalleled flexibility makes ECP a valuable tool for patients and surgeons alike, even in this age of seemingly ever-increasing MIGS options.
1. Kaplowitz K, Kuei A, Klenofsky B, Abazari A, Honkanen R. The use of endoscopic cyclophotocoagulation for moderate to advanced glaucoma. Acta Ophthalmol. 2015;93:395-401.
2. Radcliffe N, Noecker R, Sarkisian S, Parikh P. ICE surgical technique outcomes: MIGS implantation of trabecular bypass stent, cataract extraction and endoscopic cyclophotocoagulation. Paper presented at: American Glaucoma Society Annual Meeting; February 27-March 2, 2014; Washington, DC.
