




Recent advances in premium cataract surgery allow surgeons to achieve better visual outcomes for patients than was possible in the past. Due to expanding indications for surgery and rising expectations of patients, preoperative screening is a crucial step in the process of determining the right IOL for the right patient.
In the June Fundamentals in Five column, we discussed five important factors in choosing the right IOL. In this issue, we discuss five key factors that every surgeon and staff member must master in preoperative patient screening, evaluation, and counseling to ensure that patients are happy with our decisions in presbyopia-correcting surgery.

Corneal Evaluation
Corneal tomography is an effective tool to assess corneal optical quality. It provides an exhaustive examination of the corneal surface and thickness, and it can display Scheimpflug images for visualization of anterior segment structures.1 These images help to document lens opacification and make it easier to explain to patients the need for surgical intervention. The data gathered include information such as the presence of irregular astigmatism (Figure 1), corneal shape, spherical aberration, and cylinder.
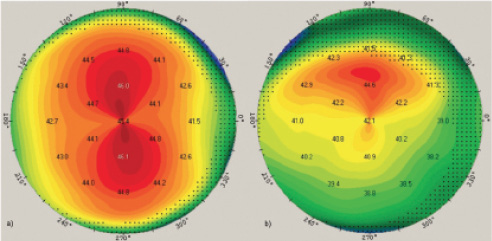
Figure 1. Corneal tomography maps showing regular (left) and irregular (right) astigmatism.
Irregular astigmatism greatly affects visual outcomes and is challenging to treat after surgery. Therefore, preoperative screening for this condition is important. Corneal tomography provides quantitative assessment of irregular astigmatism with analysis of total higher-order aberrations (HOAs), along with qualitative assessment with a refractive power map. Studies have found that patients with moderate amounts of HOAs—values greater than 0.3 µm in mild irregular astigmatism and 0.4 µm in moderate irregular astigmatism for a 4-mm pupil—are likely to experience a major decrease in visual quality postoperatively.2,3 This matters for quality of vision with presbyopia-correcting IOLs but also for asphericity and the aspheric optical profile of monofocal IOLs.
Analysis of axial power maps and the front:back corneal surface ratio in the sagittal plane allow detection of abnormalities in corneal shape. This is especially pertinent in patients with a history of refractive surgical procedures because it significantly influences IOL power calculation. Moreover, measurements of corneal spherical aberration provided by corneal tomography are essential for IOL selection and patient counseling. These measurements can help make the choice between a monofocal and an extended depth of focus (EDOF) IOL, depending on pupil size and spherical aberration.
It is also important to analyze cylinder measurements, especially if the use of toric IOLs is being considered. Measuring regular corneal astigmatism with a manual or automated keratometer is not enough. It is now mandatory to assess total HOAs in order to make the right decision. Patients with severe irregular corneal astigmatism are not eligible for toric IOL implantation. The reproducibility of tomographic cylinder measurements can be confirmed by comparing the magnitude and axis of regular astigmatism between manual keratometry and the wavefront-derived value. Several studies have shown the effect of posterior corneal curvature on visual outcomes, making these measurements important for toric IOL planning.2,4
Setting Patient Expectations
To determine the best IOL technology for patients who desire presbyopic cataract surgery, it is key to focus on each patient’s individual lifestyle and needs. Patient education and counseling helps the surgeon to decide which approach would be best. During this chair time, patients are informed about potential outcomes with an emphasis on the degree of spectacle independence that may be expected, the possibility of dysphotopic phenomena, and the potential need for postoperative refinements.
It is important to impress upon patients that presbyopia-correcting IOLs offer a wider range of vision compared to monofocal IOLs because they provide multiple foci.5 It is important to discuss with patients how their lens choices will affect their reading habits and the visual tasks required in their profession and daily activities.
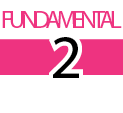
Photic phenomena are a possible side effect with presbyopia-correcting lenses, and patients must be educated about this risk by showing them images that illustrate halos and glare around light sources in different scenarios, such as driving a car at night (Figure 2). Fortunately, this side effect is rare and often disappears after a period of neural adaptation. In worst-case scenarios, surgery can be reversed and a multifocal IOL can be exchanged for a monofocal. However, it is important to remember that monofocal IOLs can also cause halos and glare.6 Patients must understand these possibilities preoperatively so that they have realistic expectations.
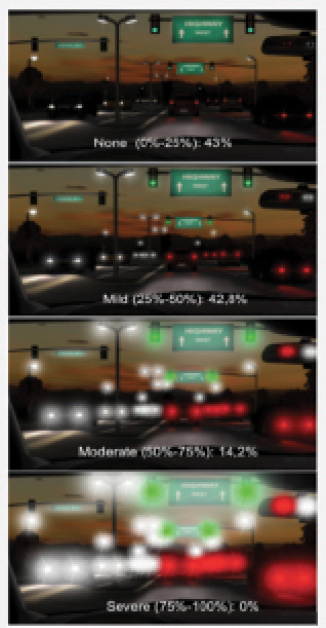
Figure 2. Halo and glare strength analysis with the AT LARA 829 EDOF IOL (Carl Zeiss Meditec).
In our practice we have learned that, with diffractive IOLs, patients need to know that they could experience halos as a result of the optical profile of the lens (Figure 3). A simple explanation can result in a happy doctor with a functional outcome and a happy patient who knew what to expect.
Figure 3. Patients can experience halos as a result of the optical profile of diffractive IOLs.
OCT Evaluation
Cataract patients generally belong to the senior population, which means that they have a relatively high rate of associated pathologies, some of which can compromise the outcomes of presbyopia-correcting IOL surgery.7 Chronic pathologies such as diabetic retinopathy and glaucoma are well documented on OCT. Other disorders that are not clinically visible can also be observed with OCT, such as mild macular edema or a transparent epiretinal membrane—either of which can negatively impact the outcomes of presbyopia-correcting surgery.
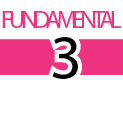
Additionally, early stages of age-related macular degeneration (AMD) can be detected on OCT. When early AMD is detected, patients should be counseled about possible chronic loss of vision in their later years after IOL implantation (Figure 4).
Figure 4. Chronic loss of vision is possible due to AMD in a patient’s later years after IOL implantation. Notice the difference in these OCT images of a regular foveal depression (top) and AMD (bottom).
Dealing With Dysphotopic Phenomena
Photic phenomena induced by the optical designs of presbyopia-correcting IOLs are often the first dissatisfaction reported by patients after premium cataract surgery.6,8 These phenomena should be discussed before surgery. Explain to patients that each optical design has a different pattern of photic phenomena, and show patients images from simulators to gauge their tolerance in the event these phenomena occur after surgery (Figure 2). Although it is not often discussed, monofocal IOLs can also cause dysphotopsia, depending on their aspheric optical profiles and especially if corneal aberrations are not taken into account.6
In bilateral presbyopia-correcting IOL surgery, when patients are motivated but undecided about their tolerance of dysphotopsia, the surgeon can implant one IOL in the nondominant eye and let the patient decide if he or she still wants the same IOL in the other eye. The latest generation of IOLs is promising with regard to the reduction of dysphotopic phenomena.6
There are also so-called mix-and-match approaches, in which two different types of IOL are used. These have been reported to result in remarkable rates of satisfaction, with significantly reduced frequency of dysphotopsia complaints by patients.9 In a small case series of older cataract patients, we found that the rate of photic phenomena in patients binocularly implanted with a rotationally asymmetric EDOF IOL with 1.50 D depth of focus at the IOL plane resulted in rates of halos and glare comparable to those in patients implanted with a monofocal IOL.10
Taking Account of Associated Disorders
In order to avoid pitfalls in premium cataract surgery, it is important to conduct an exhaustive ophthalmic examination to determine the right candidates for presbyopia-correcting surgery, eliminate those who have contraindications, and fine-tune preoperative measurements.
Dry eye disease (DED) is one of the most frequently encountered conditions in candidates for premium cataract surgery.11 In severe forms, DED can cause serious ocular surface damage, significant topographic errors, and, if not well treated, poor visual outcomes that can be falsely blamed on the surgery. Therefore, proper diagnosis and management of DED is mandatory prior to surgery to ensure patients’ postoperative satisfaction and good outcomes.
A history of previous refractive surgery may require adaptation of IOL power calculation methods, surgical steps, and follow-up treatment to achieve optimal results. Additionally, patients who wear soft or rigid contact lenses must undergo preoperative measurements only after several weeks of not wearing their lenses, in order to avoid false measurements that can affect postoperative results. Patients who use orthokeratology lenses require an even longer period of discontinued lens wear before diagnostic measurements are performed.
Patients with keratoconus should be examined closely because corneal deformation complicates IOL power calculation. Certain procedures may be helpful for patients with keratoconus, such as performing CXL before cataract surgery to strengthen the cornea and making the incision on the steep axis to help reduce astigmatism.
Finally, a history of previous infection or inflammation may call for prophylactic measures. For example, patients with a history of herpes simplex virus infection must take valaciclovir pre- and postoperatively in order to prevent recurrence of the infection, which would compromise the surgical outcomes.
CONCLUSION
Premium IOL surgery, and especially presbyopia correction, is truly one of the most amazing opportunities in our profession. Relieving patients of their dependence on glasses and contact lenses not only changes their vision, but it also offers them a better quality of life.
To achieve this goal, we must be mindful when screening patients preoperatively in order not to miss out on potential problems. Awareness of our patients’ vision as an objective parameter is only one step in finding the right solution for them. The subjective aspect of our patients’ habits and daily routine plays an even more important role.
1. Loh J. Importance of performing corneal topography before cataract surgery. US Ophthalmic Review. 2015;8(2):92-96.
2. Braga-Mele R, Chang D, Dewey S, et al. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg. 2014;40:313-322.
3. Michelson MA, Myers RA. Corneal higher order aberrations and visual dysfunction with multifocal IOLs. Paper presented at: American Society of Cataract & Refractive Surgery Annual Meeting; April 20-24, 2012; Chicago.
4. Koch D, Ali S, Weikert MP, et al. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080-2087.
5. Breyer DRH, Kaymak H, Ax T, et al. Multifocal intraocular lenses and extended depth of focus intraocular lenses. Asia Pac J Ophthalmol (Phila). 2017;6(4):339-349.
6. Tarib I, Al-kadhi R, Abdassalm S. Comparisson of visual side-effects in patients with different IOL models and phakic patients using the halo & glare simulator. Paper presented at: The 32nd Annual Conference of the DGII; February 15-17, 2018; Leipzig, Germany.
7. Moreira CA, Moreira CA, Moreira AT. Optical coherence tomography in patients undergoing cataract surgery. Arq Bras Oftalmol. 2015;78(4):241-245.
8. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992-997.
9. Kretz F, Breyer D, Abdassalam S, et al. Enhancing intermediate vision and patient satisfaction by combining an enhanced depth of focus IOL and a trifocal IOL model. Paper presented at: The 31st Annual Meeting of the Asia-Pacific Association of Cataract & Refractive Surgeons; July 19-21, 2018; Chiang Mai, Thailand.
10. Tarib I, Kretz F. Benefits of a rotationally asymmetric enhanced depth of focus, bifocal segment intraocular lens in an older cataract population ranging from 74 to 82 years. EC Ophthalmology. 2018;9(5):248-256.
11. Afsharkhamseh N, Movahedan A, Motahari H, et al. Cataract surgery in patients with ocular surface disease: an update in clinical diagnosis and treatment. Saudi J Ophthalmol. 2014;28(3):164-167.



