



The importance of astigmatism correction at the time of cataract surgery increases as patient demand for excellent postoperative vision grows. Predicting the magnitude and axis of astigmatism, however, is limited by the variable accuracy of posterior corneal measurements and, more importantly, postoperative healing.
Traditionally, residual astigmatism has been managed with spectacles, limbal relaxing incisions, corneal refractive surgery, and IOL exchange. Most of these approaches entail additional surgical risk, and all of them require time and may leave the patient and physician frustrated. An advantage of a Light Adjustable Lens (LAL; RxSight) is it allows astigmatism to be corrected based on the patient’s postoperative manifest refraction instead of preoperative calculations. The foldable three-piece LAL is composed of photosensitive silicone, and multiple refractive adjustments with UV light may be performed before the final power is locked in.
MY APPROACH TO ASTIGMATISM CORRECTION
Primary candidates. I favor the LAL in situations where the accuracy of the IOL calculation is questionable (eg, patients with a history of refractive surgery) and where the goal is sharp visual acuity with minimal risk of postoperative glare and halos. Approximately 2.00 D of sphere or cylinder can be corrected per light treatment. I find that the maximum amount of total astigmatism correction with an LAL is about 2.50 to 3.00 D.
In a review of the first 54 eyes at my practice to receive an LAL with ActivShield technology, the magnitude of astigmatism on manifest refraction decreased from 0.79 ±0.70 D before the first light treatment of the LAL to 0.13 ±0.29 D at the final lock-in, usually 6 weeks after surgery (Figure 1).1 Of the 54 eyes, 26 (48%) had previously undergone corneal refractive surgery, and 79% achieved a result within ±0.25 D of the spherical refractive target.
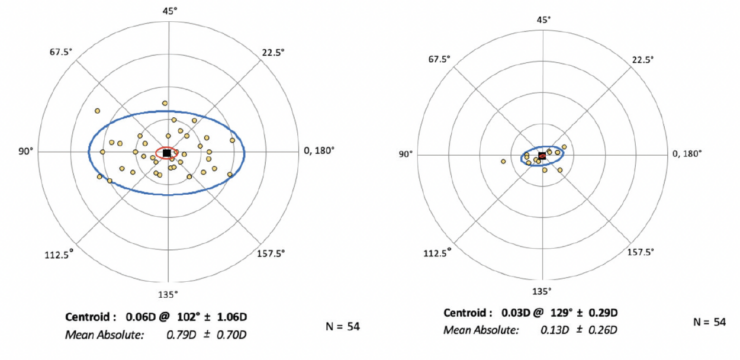
Figure 1. The mean absolute decrease of the magnitude of astigmatism from before the first light treatment of the LAL to the final lock-in.
High regular astigmatism. I find the LAL to be the most accurate option for eyes with low to moderate regular astigmatism. I favor toric IOLs for eyes with high regular astigmatism because the axis and magnitude tend to be easier to predict.
Irregular astigmatism. The LAL may be a good option in this situation, particularly if the patient is unable to tolerate a rigid gas permeable contact lens to attain optimal vision. The implantation of an LAL could potentially diminish their postoperative astigmatism to a degree sufficient to optimize vision without requiring a contact lens.
CASE EXAMPLE: KERATOCONUS
A 67-year-old man with long-standing keratoconus presented for a cataract surgery evaluation. The patient had attempted to wear rigid gas permeable and scleral contact lenses in the past but could not tolerate either owing to difficulty with the lenses’ daily removal. He was therefore motivated to reduce his manifest refraction as much as possible.
The patient’s glasses prescription had not changed significantly during the past several years. Topography showed inferior steepening consistent with keratoconus in each eye (Figure 2). Measurements with the IOLMaster (Carl Zeiss Meditec) showed 3.60 D of astigmatism OD and 7.50 D OS (Figure 3).

Figure 2. Topography showing inferior steepening consistent with keratoconus in the right (A) and left (B) eyes.
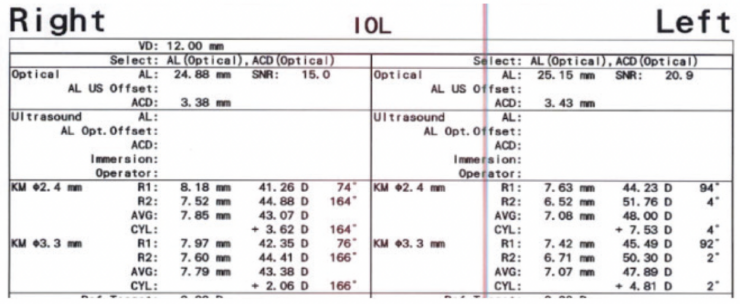
Figure 3. Measurements with the IOLMaster showed 3.60 D of astigmatism OD and 7.50 D OS.
IOL calculations were performed with the Kane KCN formula, and a plano result was targeted in both eyes. An LAL was implanted bilaterally.
At the time of the first light adjustment, the patient’s BCVA was 20/25-2 OD with a manifest refraction of +2.25 -2.75 x 75º. His UCVA was 20/300 OS, and his BCVA was 20/30 OS with a manifest refraction of +4.00 -2.75 x 65º. After the third and final light adjustment of the LAL in each eye, his BCVA was 20/25-2 OD with a refraction of +0.50 -1.00 x 100º. His UCVA was 20/80 OS, and his BCVA was 20/30 OS with a refraction of +1.75 -2.25 x 100º. Interestingly, the magnitude of astigmatism in the left eye was significantly lower than preoperative biometry had suggested, which underscores the unpredictable impact of the posterior cornea in eyes with ectasia or an irregular cornea.
The patient was able to drive without spectacle correction. He wore prescription readers for near tasks.
1. Stephens JD. Paper presented at: The Caribbean Eye Meeting; February 4–7, 2022; Rio Grande, Puerto Rico.
