


Sometimes, manually marking the eye for toric IOL implantation is the right call
By Akaanksh Shetty, MD, and Rahul S. Tonk, MD, MBA


Toric IOLs are vital to maximizing refractive outcomes in cataract surgery. Success with the technology hinges on accurate preoperative measurements, the management of surgically induced astigmatism, precise alignment of the IOL on the target axis, and the mitigation of postoperative IOL rotation.
This article provides pearls for the accurate intraoperative identification and marking of the desired target axis with manual ink marks. It also makes the case for using manual marks—at least occasionally—in an age of digital, markerless devices.
MANUAL MARKING: OUR TECHNIQUE
Accurately marking the target toric IOL axis requires compensating for cyclotorsion and making marks that are sufficiently thin and remain visible through sterile preparation and surgery. Compensating for cyclotorsion typically involves marking a reference axis preoperatively (while the patient is in an upright position) and then using this reference intraoperatively (while the patient is supine) to identify and mark the target toric IOL axis.1
Preoperative reference marks. There are many different techniques and instruments for creating marks manually. The protocol we have found helpful is presented in the sidebar Our Protocol for Manual Marking. We routinely mark the eye at the patient’s bedside while they are in the preoperative holding area. Some surgeons find that marking at the slit-lamp microscope gives them greater control.2
Our Protocol for Manual Marking
No. 1: Familiarize the patient with a predetermined distance fixation target to ensure their comfort and cooperation.
No. 2: Seat the patient upright and ensure that their head is straight.
No. 3: Apply a drop of a topical anesthetic.
No. 4: Open the patient’s eyelids with two fingers or, if they are prone to blinking, a comfortable eyelid speculum.
No. 5: Thoroughly dry the areas you wish to mark using a cotton-tipped applicator or Weck-Cel sponge (BVI Medical).
No. 6: Confirm patient fixation is on target.

Figure 1. Reference axes are marked at the 3, 6, and 9 clock positions with a three-bladed toric marker.
No. 8: Dry the marks before the patient blinks to avoid smudging.
No. 9: Confirm proper visibility and alignment of reference marks and make adjustments as necessary (Figure 2).

Figure 2. Reference axis marks are reinforced to increase their visibility.
We favor a reusable stamp marker (Vann Toric marker ET-03, Ambler Surgical; Figure 1 in the sidebar on manual marking), which marks the limbus at the 3, 6, and 9 clock positions. Other surgeons may prefer to make marks freehand with a fine-tipped marker such as the Blephmarker (Viscot Medical) or a device such as the Davis MD OneStep (Mastel Precision), RoboMarker System (Surgilūm), or Wet-Field Osher Thermodot Marker (BVI Medical). Regardless, it is critical to mark the corneal edge of the limbus to some extent because marks on the conjunctival edge may be obscured by subconjunctival hemorrhage and chemosis.
Correct horizontal alignment of the reference marks can be confirmed visually or with a smartphone application such as toriCAM (Graham Barrett) on the Apple operating system and iToric (Dr. Sourabh D. Patwardhan) on Android.3,4
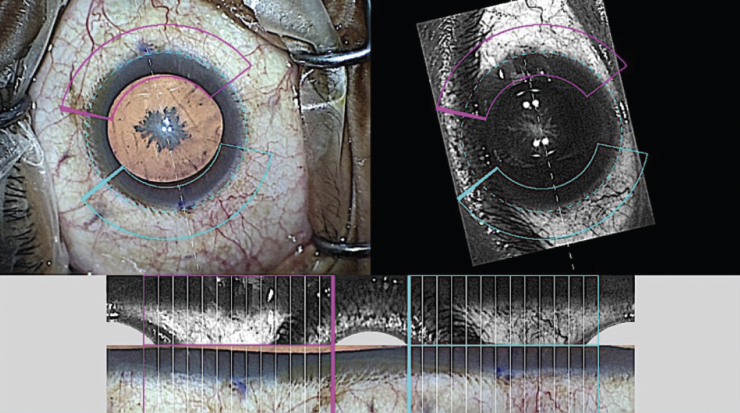
Figure 1. Callisto eye determines the horizontal axis (dotted white line, top panel) by comparing it with a preoperative reference image of conjunctival-limbal blood vessels (bottom panel). Note that the horizontal axis coincides with the manual reference marks nasally and temporally (purple dots).
Figures 1–3 and sidebar figures courtesy of Rahul S. Tonk, MD, MBA
Intraoperative target axis marks. The steps for marking the target axis intraoperatively are presented in the sidebar Intraoperative Marking of the Target Axis. Several instruments may be used to mark the target axis. We favor the Cionni Toric Axis Marker (Duckworth & Kent; Figure 1 in the sidebar on intraoperative marking) but also like the Koch-Mendez degree gauge and Henderson Toric IOL Marker (both instruments available from various manufacturers), which offer the added benefit of globe stabilization.
We prefer to mark the target axis at the start of surgery when the globe is closed, the reference marks are clearly visible, topical anesthesia is maximal, and there is minimal to no conjunctival chemosis. Target axis marks are made peripherally enough that they do not obstruct visualization during surgery.
Intraoperative Marking of the Target Axis
Step No. 1: Prepare and drape the patient in the usual sterile manner.
Step No. 2: Identify the preplaced reference marks.
Step No. 3: Mark the target IOL axis relative to the reference marks with your instrument of choice (Figure 1).
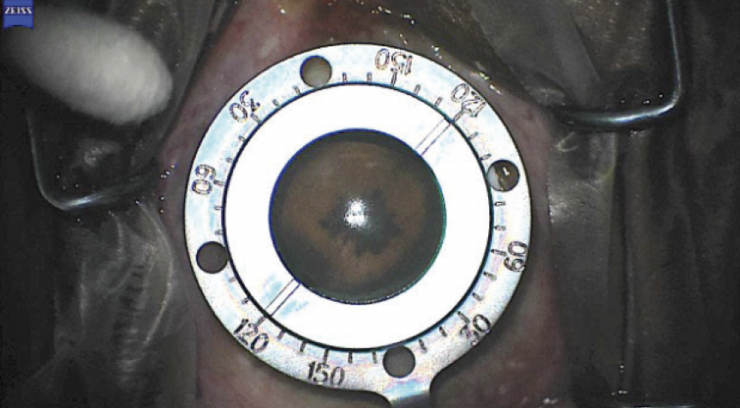
Figure 1. A Cionni Toric Axis Marker (Duckworth & Kent) is aligned with the reference marks at 0º and 180º. The instrument is then applied to the cornea to mark the target axis (122º).
Step No. 4: Proceed with surgery. Align the toric IOL along the target axis (Figure 2).
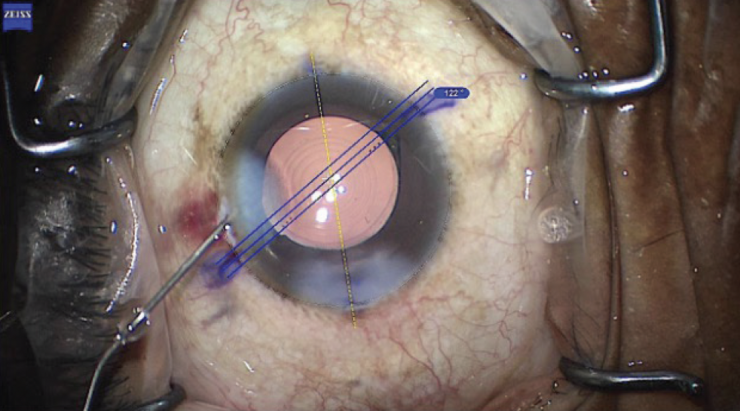
Figure 2. Final toric IOL alignment. The IOL marks, digital target axis overlay, and manual target axis marks are all in agreement.
DIGITAL VERSUS MANUAL MARKING
Manual marking is increasingly being supplanted by digital marking systems such as Callisto eye (Carl Zeiss Meditec; Figures 1 and 2), the Verion and ORA Systems (Alcon), IntelliAxis Refractive Capsulorhexis for the Lensar Laser System (Lensar), and Cassini (i-Optics) on the Catalys Precision Laser System (Johnson & Johnson Vision). Several studies have shown that digital systems can improve IOL alignment and even occasionally reduce postoperative residual astigmatism. No controlled study to date, however, has been able to demonstrate an actual improvement in visual acuity with digitally versus manually marked eyes.5,6
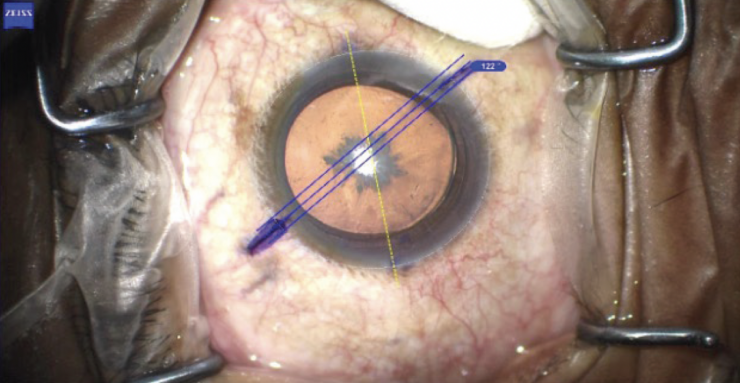
Figure 2. Manual marks and Callisto eye overlay (blue lines) agree on the target axis (122º).
For some practices, the acquisition of a digital system may not be cost-effective or practical, particularly if it requires the purchase of a reference imaging device such as a topographer or biometer that is redundant with current equipment.
There are situations, moreover, where a digital marking system may fail:
- A reference image cannot be captured or uploaded preoperatively (eg, featureless eyes, network error);
- A reference image cannot be registered intraoperatively, such as in instances of progressive conjunctival chemosis (Figure 3) or with alterations in iris illumination or configuration;
- The patient cannot tolerate or be positioned for a marking system that requires a femtosecond laser; and
- Intraoperative corneal edema affects the quality of optical wavefront aberrometry.
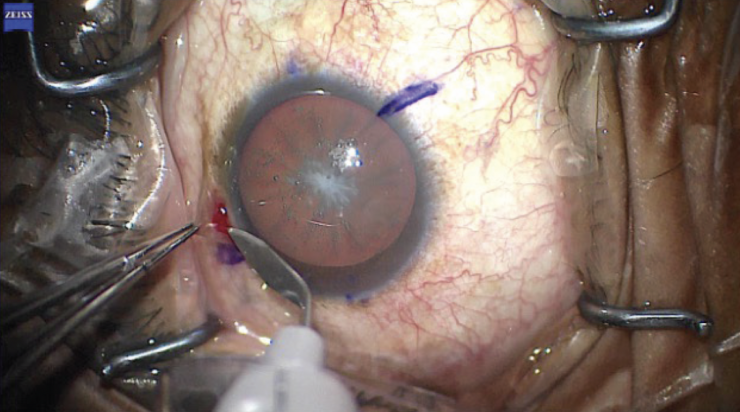
Figure 3. Chemosis of the conjunctiva is reduced to prevent obscuration of the conjunctival limbal reference marks that are necessary for the Callisto eye registration software.
These occasional drawbacks notwithstanding, we routinely use digital marking devices because of their precision and predictability. Nonetheless, we frequently employ manual marks when digital marking technology is not available or may be affected adversely by intraoperative conditions.
Whatever the marking style, what matters most is the surgeon’s willingness to manage astigmatism and improve patients’ refractive outcomes.
1. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631-1636.
2. Ding N, Wang X, Song X. Digital versus slit-beam marking for toric intraocular lenses in cataract surgery. BMC Ophthalmol. 2022;22(1):323.
3. Khatib ZI, Haldipurkar SS, Shetty V. Verion digital marking versus smartphone-assisted manual marking and isolated manual marking in toric intraocular lens implantation. Indian J Ophthalmol. 2020;68(3):455-458.
4. Pallas A, Yeo TK, Trevenen M, Barrett G. Evaluation of the accuracy of two marking methods and the novel toriCAM application for toric intraocular lens alignment. J Refract Surg. 2018;34(3):150-155.
5. Webers VSC, Bauer NJC, Visser N, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Image-guided system versus manual marking for toric intraocular lens alignment in cataract surgery. J Cataract Refract Surg. 2017;43(6):781-788.
6. Elhofi AH, Helaly HA. Comparison between digital and manual marking for toric intraocular lenses: a randomized trial. Medicine (Baltimore). 2015;94(38):e1618.
A review of currently available image-guided systems for astigmatism management in cataract surgery
By Mahipal S. Sachdev, MD, and Pranita Sahay, MD, FRCS (Glasgow), FRCOphth, FICO (Cornea), FAICO (Ref Sx)


Nearly one-third of patients undergoing cataract surgery have greater than 1.00 D of corneal astigmatism.1 It is therefore not surprising that the popularity of toric IOLs increased dramatically during the past decade. Shimizu et al2 introduced the concept of a toric IOL in 1992. Proper axial marking helps increase the accuracy of toric IOL alignment and improve visual outcomes. Marking techniques have evolved from early manual approaches (Figure 1 in Our Protocol for Manual Marking and Intraoperative Marking of the Target Axis) to iris fingerprinting (introduced by Osher et al1 in 2010) and beyond. This article highlights the usefulness of current noncontact image-guided systems.
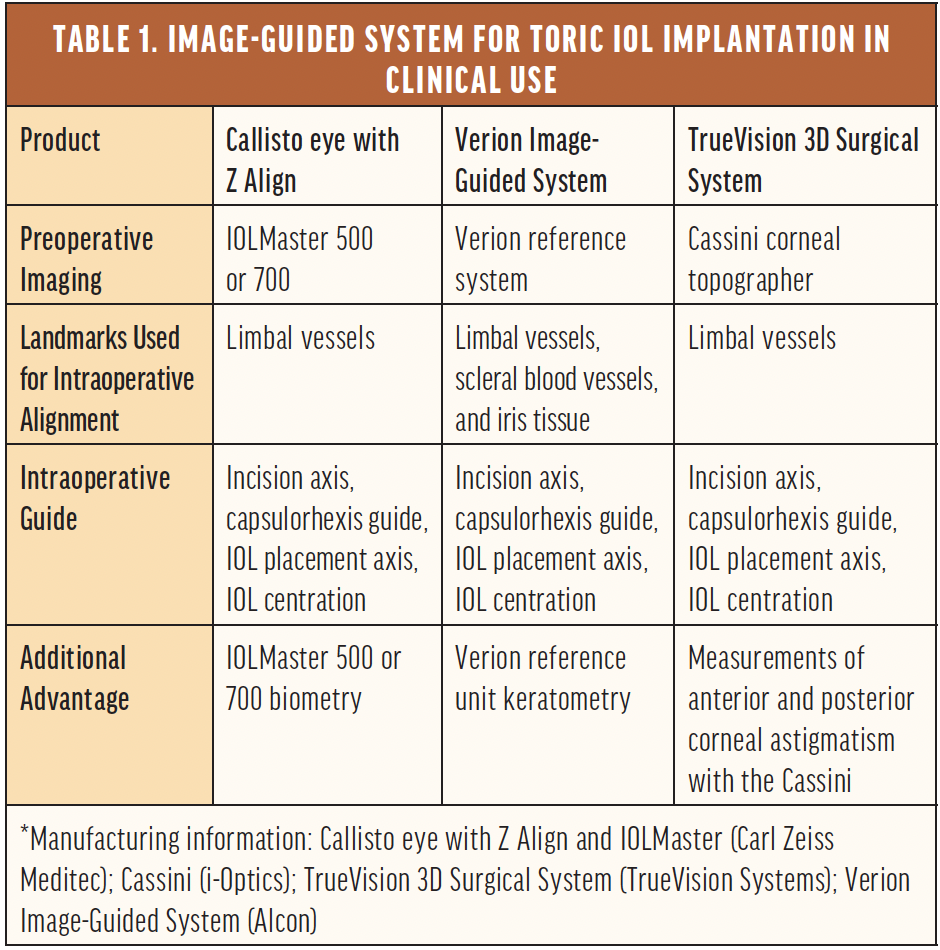
IMAGE-GUIDED MARKING SYSTEMS
Technologies currently available for clinical use (Table 1) include Callisto eye with Z Align, the Verion Image‐Guided System, and the TrueVision 3D Surgical System (TrueVision Systems). The Callisto and TrueVision systems use only limbal vessels as landmarks for identifying the eye’s position, whereas the Verion also uses scleral vessels and iris tissue.
A preoperative image of the eye is captured and matched with an intraoperative image to compensate for cyclotorsion due to the supine positioning of the patient (Figures 4 and 5). All three systems project a reference (0º–180º) and target axis (IOL implantation axis) during surgery (Figure 2 in Intraoperative Marking of the Target Axis). The platforms may be used to assist with the alignment of both toric and phakic toric IOLs.
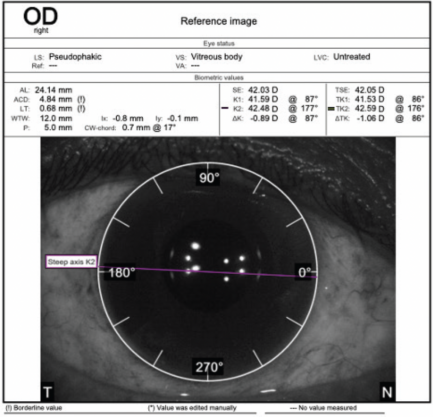
Figure 4. Preoperative reference image captured with the IOLMaster 700.
Figures 4-6 courtesy of Mahipal S. Sachdev, MD
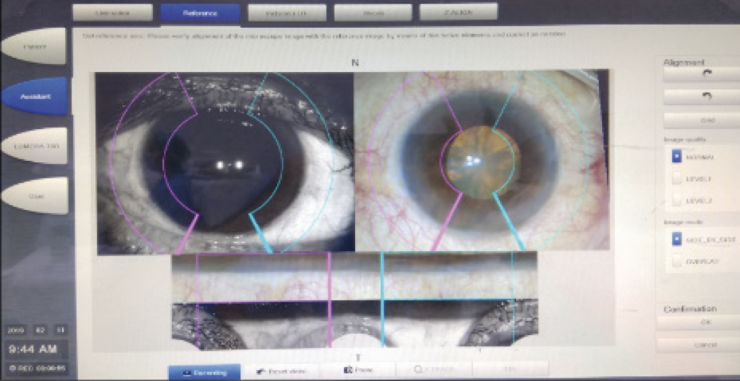
Figure 5. Matching of the intraoperatively captured image and reference image with Callisto eye with Z Align.
Femtosecond laser platforms can also assist with astigmatism management. For example, intraoperative iris registration with the Catalys Precision Laser System and Lensar Laser System facilitates the creation of intrastromal corneal incisions (Figure 6), and the Lensar can be used to mark the lens capsule for toric IOL alignment. Recent integration of the cOS 7.0 software into the Catalys allows preoperative patient data from the IOLMaster 700 (Carl Zeiss Meditec) to be imported automatically.
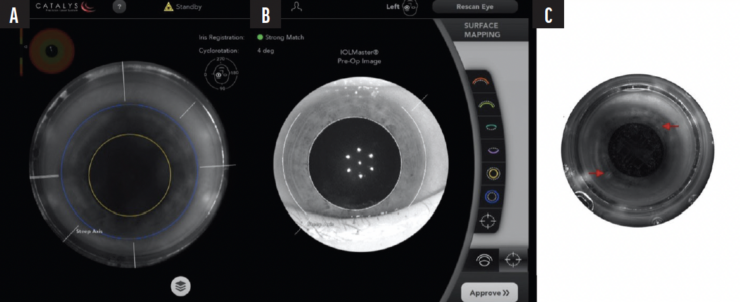
Figure 6. The steep corneal axis is marked for toric IOL implantation with the Catalys in an eye that will undergo laser cataract surgery (A). Intraoperative iris registration and matching with the IOLMaster using cOS 7.0 software (B). An intrastromal corneal incision (red arrows) is made at the target axis with a femtosecond laser (C).
Pointers for Success
The success of toric IOL surgery depends primarily on the alignment of the IOL. Following are four pointers for success when performing the procedure with an image-guided system.
No. 1: Ensure the patient’s head is properly positioned (ie, no tilt) when capturing an image of the eye preoperatively.
No. 2: Check the data transfer on the intraoperative imaging system before shifting the patient to the OR to avoid data loss.
No. 3: If block anesthesia is planned, consider marking the eye manually as a backup measure. This precaution can save the day if the image-guided system is unable to capture an image intraoperatively owing to conjunctival chemosis or subconjunctival hemorrhage, for example.
No. 4: Intraoperatively align the toric IOL marks with the projected axis to avoid misalignment and horizontal displacement of the lens.
ADVANTAGES
The transition from conventional/manual marking to an image-guided/digital system can increase patient comfort and improve visual outcomes. For instance, smudged ink, irregular and overly thick marks, and faded ink are avoided. Image-guided systems can also be helpful when patient cooperation is poor.
Toric IOL calculations take biometry measurements and data on surgically induced astigmatism into account. Image-guided systems help identify the best axis for implantation of a toric IOL and a reference axis for incision placement. They also provide an intraoperative capsulorhexis guide to improve centration and sizing.
DISADVANTAGES
Pre- and intraoperative image registration is an essential step to estimating the eye’s position and guiding axial alignment. In some cases, the eye tracker disengages multiple times, necessitating repeated registration. The risk of registration problems increases in the presence of conjunctival chemosis, ballooning, and bleeding; poor patient cooperation; deep-set eyes; and a narrow palpebral aperture. Proper preoperative planning is essential, particularly when block anesthesia will be required for cataract surgery because it can cause conjunctival chemosis and subconjunctival hemorrhage.
Additionally, a major disadvantage of image-guided systems is their cost.
MANUAL VERSUS IMAGE-GUIDED MARKING
Several studies have compared the utility and benefits of image-guided toric IOL implantation versus the manual method of marking (bubble marker/slit-beam marking).3-6 Most of the studies suggested that the degree of axial misalignment and amount of postoperative residual cylinder may be lower with the image-guided method, but the anatomic benefit did not translate into better postoperative UCVA. Titiyal et al reported better vision quality (eg, modulation transfer function and Strehl ratio) but comparable visual acuity.6 A meta-analysis found that image-guided marking resulted in less axial misalignment, a smaller difference vector, and less postoperative astigmatism.7
CONCLUSION
Image-guided systems can increase the accuracy of a toric IOL’s axial alignment. The technology can be a beneficial addition to surgeons’ offerings if its cost is not prohibitive.
1. Singh VM, Ramappa M, Murthy SI, Rostov AT. Toric intraocular lenses: expanding indications and preoperative and surgical considerations to improve outcomes. Indian J Ophthalmol. 2022;70(1):10-23.
2. Kaur M, Shaikh F, Falera R, Titiyal J. Optimizing outcomes with toric intraocular lenses. Indian J Ophthalmol. 2017;65(12):1301-1313.
3. Webers VSC, Bauer NJC, Visser N, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Image-guided system versus manual marking for toric intraocular lens alignment in cataract surgery. J Cataract Refract Surg. 2017;43(6):781-788.
4. Kodavoor SK, Divya J, Dandapani R, Ramamurthy C, Ramamurthy S, Sachdev G. Randomized trial comparing visual outcomes of toric intraocular lens implantation using manual and digital marker. Indian J Ophthalmol. 2020;68(12):3020-3024.
5. Ding N, Wang X, Song X. Digital versus slit-beam marking for toric intraocular lenses in cataract surgery. BMC Ophthalmol. 2022;22(1):323.
6. Titiyal JS, Kaur M, Jose CP, Falera R, Kinkar A, Bageshwar LM. Comparative evaluation of toric intraocular lens alignment and visual quality with image-guided surgery and conventional three-step manual marking. Clin Ophthalmol. 2018;12:747-753.
7. Zhou F, Jiang W, Lin Z, et al. Comparative meta-analysis of toric intraocular lens alignment accuracy in cataract patients: Image-guided system versus manual marking. J Cataract Refract Surg. 2019;45(9):1340-1345.
