



Spectacle independence has become a point of focus for individuals undergoing cataract and refractive lens exchange surgeries. It is common for patients to present to an eye care provider after conducting online research and ask to receive a specific IOL. Residual astigmatism is the main reason for patients’ postoperative dissatisfaction.1,2 This article describes how I have leveraged customized toric IOLs to build a successful refractive surgery practice in Perth, Western Australia.
A FEW WORDS ABOUT PERTH
Perth is the fourth largest city in Australia, but it is regarded as the most competitive urban market for refractive and vision correction surgery in the country. The population of Perth is one-third that of Sydney or Melbourne, yet it has twice the number of practices with excimer lasers per capita. Further, more femtosecond lasers that can be used to perform lenticular extraction (SMILE) are located in Perth than in Sydney and Melbourne combined.
I set up my refractive surgery practice in early 2019. Other more well-established centers in Perth offer lens extraction for vision correction. Achieving success required differentiating my practice from theirs. Offering patients customized IOLs made my practice less reliant on standard retail lenses.
OPTIMIZING REFRACTIVE OUTCOMES
Advances in IOL power calculations (for both spherical and cylindrical errors) and designs challenged me to look beyond simply restoring patients’ visual acuity to optimizing refractive outcomes.3 Full spectacle independence became a more achievable goal with the release of the most recent extended depth of focus and multifocal IOL designs, but success with these lenses depends on how well patients’ corneal astigmatism is managed.
Australia’s Public Health Service, Medicare, and health insurance programs cover the use of toric IOLs. Patients can therefore realistically expect to achieve exceptional refractive outcomes without incurring an out-of-pocket expense. The closer the postoperative refraction is to plano, the better the patient’s UCVA is. Even a tiny amount of residual cylinder can affect quality of vision.3-7
I favor the Lentis family of IOLs (Teleon Surgical) for patients who have at least 0.50 D of preexisting corneal astigmatism. These IOLs are available in three add powers and can be customized in 0.01 D steps for sphere and cylinder (Figures 1–3). Most other retail lenses offer astigmatic correction only in units of 0.50 or 0.75 D.
I have implanted a customized toric IOL to correct less than 0.30 D of preexisting cylinder. My goal is to correct astigmatism with accuracy comparable to what can be achieved with an excimer laser. In a recent study of 90 eyes of 48 patients, I evaluated the accuracy of astigmatic correction after the implantation of customized toric IOLs (Figure 4). All patients had a postoperative visual acuity of 0.0 logMAR or better. The amount of corneal astigmatism corrected ranged from 0.27 to 4.98 D. The mean amount of postoperative refractive astigmatism was 0.31 D.

Figure 1. Sample customized IOL printout with a low astigmatic correction (0.27 D).

Figure 2. Sample customized IOL printout with a high astigmatic correction (3.93 D). Both sphere and cylinder are available in 0.01 D steps.
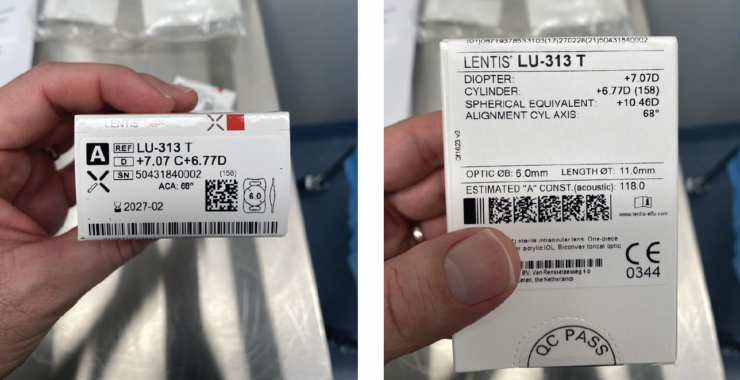
Figure 3. Examples of customized toric IOLs.
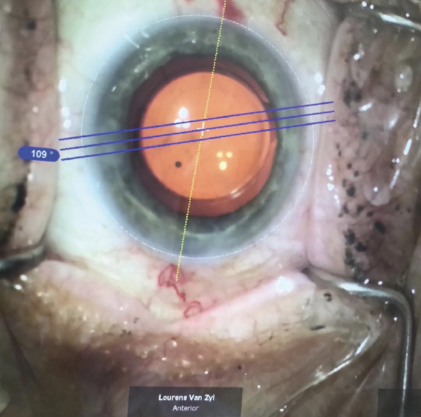
Figure 4. Placement of a customized toric lens under electronic guidance from the Callisto eye platform (Carl Zeiss Meditec).
Forty of the eyes had a postoperative manifest refraction of plano and a mean absolute prediction error of 0.32 D. Ninety-four percent of operated eyes were within ±0.50 D of the predicted cylindrical outcome of 0.00 D. Manifest refraction showed that 44% of eyes had no measurable refractive error postoperatively; among those with a measurable refractive error, it was no more than 0.50 D in most cases. Most of the patients with residual refractive errors had 2.50 D or more of oblique corneal astigmatism before surgery.6
CONCLUSION
In less than 5 years, my practice has become a top destination for vision correction surgery in Perth because it is the only one to offer customized toric IOLs. This correction strategy with standard monofocal and extended depth of focus Lentis toric IOLs can benefit even patients with high astigmatism, including those with a history of corneal transplantation and lacerations. When the postoperative UCVA of these patients is 0.0 logMAR and almost all their astigmatism has been corrected, they are typically ecstatic.
1. Mojzis P, Peña-García P, Liehneova I, Ziak P, Alió JL. Outcomes of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2014;40(1):60-69.
2. Law EM, Aggarwal RK, Kasaby H. Clinical outcomes with a new trifocal intraocular lens. Eur J Ophthalmol. 2014;24(4):501-508.
3. Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19:524-533.
4. Goggin M, Zamora-Alejo K, Esterman A, van Zyl L. Adjustment of anterior corneal astigmatism values to incorporate the likely effect of posterior corneal curvature for toric intraocular lens calculation. J Refract Surg. 2015;31(2):98-102.
5. Goggin M, van Zyl L, Caputo S, Esterman A. Outcome of adjustment for posterior corneal curvature in toric intraocular lens calculation and selection. J Cataract Refract Surg. 2016;42(10):1441-1448.
6. Sheen-Ophir S, LaHood B, Goggin M. Refractive outcome of toric intraocular lens calculation in cases of oblique anterior corneal astigmatism. J Cataract Refract Surg. 2020;46(5):688-693.
7. LaHood BR, Goggin M, Esterman A. Assessing the likely effect of posterior corneal curvature on toric IOL calculation for IOLs of 2.50 D or greater cylinder power. J Refract Surg. 2017;33(11):730-734.