


From Ink Marks to Digital Technologies
Gilles Lesieur, MD, and Paul Dupeyre, MSc


From 2016 to 2022, the toric IOL implantation rate increased in Europe, from 7% to 15%, respectively.1 Misalignment of these lenses reduces their efficacy.
In a 2019 survey of clinical trends conducted by the ESCRS,2 manual ink marking was the preferred method for orienting a toric IOL to the intended axis (Figure 1). Forty-one percent of respondents reported making ink marks with the aid of manual axial instruments. Digital image registration was used by 22% of respondents. (For more on this subject, see Manual and Image-Guided Techniques: Optimizing Toric IOL Implantation.)
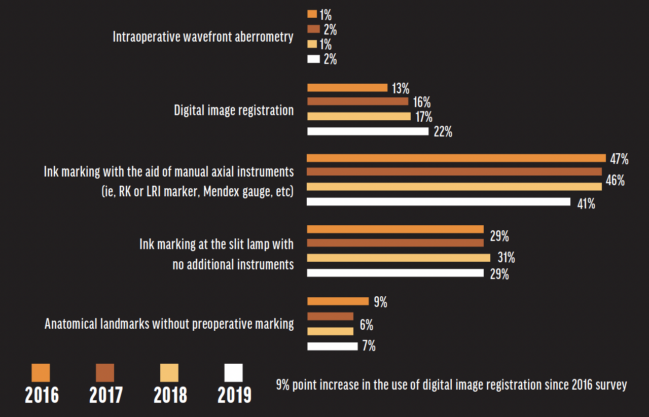
Figure 1. ESCRS Clinical Trends Survey 2022 Results: Preferred options for aligning a toric IOL with the intended axis.2
Abbreviations: RK, radial keratotomy; LRI, limbal relaxing incision
Figures 1 and 2 courtesy of Gilles Lesieur, MD
Problems with ink marks are that they can fade and their thickness can lead to IOL misalignment. Digital registration can offer greater speed, security, and precision. Several tools are available, and their use has become more common.
OVERVIEW of SYSTEMs (IN ALPHABETICAL ORDER)
Callisto eye (Carl Zeiss Meditec). This markerless toric IOL alignment system connects with the Zeiss Cataract Suite (Carl Zeiss Meditec). The assistance functions selected during biometry are transferred directly to the oculars of the surgical microscope and matched to the patient’s eye. Automated eye tracking helps ensure proper positioning of the digital marks (Figure 2).
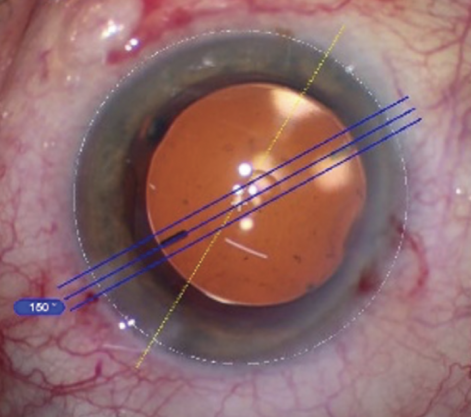
Figure 2. Alignment with Callisto eye.
Illuminated Surgical Keratoscope (Mastel). This device is mounted to the objective lens of the surgical microscope. The keratoscope has a flashing fixation target and three concentric rings of illuminating LED lights arranged every 10º. According to the company, the LED array can show corneal astigmatism down to 1.00 D or less, which can help minimize errors in toric IOL alignment and the placement of relaxing incisions.
ORA System with VerifEye+ Technology and the Verion Image Guided System (Alcon) and IntelliAxis-L (Lensar). This is a suite of integrated surgical planning and digital guidance technologies. Verion automatically matches preoperative registration marks with anatomic landmarks such as scleral vessels, the limbus, and the pupil. Intraoperative aberrometry with the ORA System can provide real-time optimization of sphere and cylinder correction.
A retrospective case series found that toric IOL alignment was better in eyes for which the image-guided system was used compared to a manual marking method.3 Improvements in postoperative uncorrected distance visual acuity or residual refractive astigmatism with digital marking generally have not been observed.4,5
IntelliAxis-L for the Lensar Laser System (Lensar) identifies the location of the steep corneal axis at the capsular plane for intra- and postoperative toric IOL alignment. The marks remain visible after surgery, which can help surgeons identify postoperative rotation of the IOL and guide its realignment.
RoboMarker System (Surgilūm). This self-leveling corneal marker has pre-inked, sterile, disposable tips. A concealed gravity-based system allows the ring dial to maintain the chosen axis to within 1º, according to the company. The ink is a dry formula to prevent smudging when applied to the cornea, and marks can last for up to 2 hours. An integrated fixation light can facilitate positioning of the eye in addition to giving patients a focal point to look at.
T-Cone Toric Platform with EyeSuite Toric Planner and Tocular (Haag-Streit). The T-Cone Toric Platform for the Lenstar (Haag-Streit) provides 11-ring Placido topography—data surgeons may use to check the symmetry and regularity of astigmatism and confirm axial location. The EyeSuite Toric Planner is part of the T-Cone Toric Platform. With EyeSuite, users can plan surgery on high-resolution images of the eye. The planner’s incision optimization tool helps minimize residual astigmatism. Surgical planning sketches based on the high-resolution images may be printed and hung near the microscope.
Tocular (Haag-Streit) is a rotatable wide-angle ocular with an integrated reticle. After a toric IOL is implanted, the reticle is turned to align the large-scale marks with the ink marks on the eye. The IOL is then positioned.
TrueGuide (TrueVision 3D Surgical). This computer-generated surgery system projects templates on the live surgical field of view to aid toric IOL alignment and incision placement. The software has been integrated into the Lensar Laser System (Lensar).
1. Nuijts MMA R. ESCRS Clinical Trends Survey 2022 Results. Eurotimes. 2023(5);28;20-21.
2. Kerr C. ESCRS Clinical Trends Survey 2019 Results. November 5, 2020. Accessed May 17, 2023. https://www.escrs.org/eurotimes-articles/escrs-clinical-trends-survey-2019-results
3. Ohashi T, Kojima T. Comparison of the orientation of the corneal steep meridian determined by image-guided system and manual method in the same eye. Clin Ophthalmol. 2020;14:4135-4144.
4. Lesieur G. Efficacité comparée du positionnement d’un implant torique de micro incision avec et sans marquage avec injection d’image. SFO-Online-Société Française d’Ophtalmologie. 2015. Accessed May 17, 2023. https://www.sfo-online.fr/session/media/efficacite-comparee-du-positionnement-dun-implant-torique-de-micro-incision-avec-et
5. Webers VSC, Bauer NJC, Visser N, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Image-guided system versus manual marking for toric intraocular lens alignment in cataract surgery. J Cataract Refract Surg. 2017;43(6):781-788.
cOS 7.0 for the Catalys Precision Laser System
By Erik L. Mertens, MD, FEBO, FWCRS

I was the first ophthalmologist worldwide to trial cOS 7.0, the latest software upgrade to the Catalys Precision Laser System (Johnson & Johnson Vision). New features that address astigmatism management and enhance workflow have expanded the platform’s capabilities beyond capsulotomy and lens fragmentation.
UPDATES
cOS 7.0, now synchronized with the IOLMaster 700 (Carl Zeiss Meditec), enables automatic data importation at the push of a button. I found it greatly increased procedural speed and enhanced the surgical experience by significantly reducing data entry and transcription errors.
I was pleased to find both the Stevens and Donnenfeld arcuate keratotomy nomograms included. The addition increases users’ ability to tailor surgery to their incision preferences.
Precision and accuracy are fundamental to positive patient outcomes with toric IOLs, and cOS 7.0 delivers on both counts by providing easily visualized toric alignment marks at the push of a button (Figure 3). My team appreciated the enhancements in workflow management, particularly the elimination of manual tasks. Specifically, they no longer needed to manually export the toric alignment marks or use a pen to mark the horizontal axis at the slit lamp. In addition to these workflow improvements, the latest software includes cybersecurity upgrades and remote monitoring with improved AI algorithms, helping predict maintenance schedules to avoid unexpected system downtime.
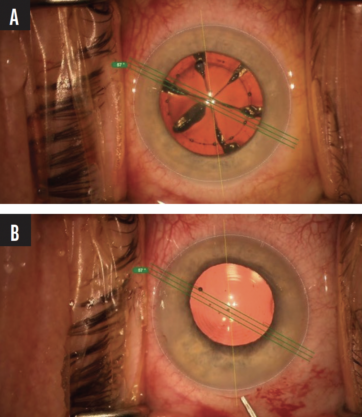
Figure 3. The lens after successful chopping and capsulotomy with digital toric alignment marks (A). The eye of the same patient after toric IOL implantation showing alignment of the digital toric marks and the measurements (B).
In every case, I was either satisfied or very satisfied with the cOS 7.0 workflow. The importation of data from the IOLMaster 700 and iris registration were successful in 57 of 58 cases. I was satisfied in all instances when nomograms and toric marks were used.
CONCLUSION
My mission is to transform patients’ lives through medical excellence, and it is for this reason that I embrace innovative technologies such as laser cataract systems. These platforms were developed to improve the standardization of care, limit the risk associated with human error in surgery, and move the field toward robot-assisted surgery. AI can complement the skills of ophthalmologists and improve patient outcomes.
cOS 7.0 elevated my practice in minimal time. The software was not only user-friendly but also easy to learn and integrate into our existing systems.