




Despite advances in lasers and IOLs for refractive and cataract surgery, some patients are left with residual ametropia—particularly astigmatism. There are many options for how to proceed, and the approach should be tailored to the individual situation.
SOURCES OF RESIDUAL ASTIGMATISM
Residual astigmatism after corneal refractive surgery can result from patient-related factors. For example, refractive predictability tends to be lower in patients with high versus low preoperative refractive errors.1,2 Because the procedures are more likely to be performed on eyes with a high refractive error, residual astigmatism is more common after LASIK or SMILE compared to surface ablation.3
External factors such as inaccurate preoperative measurements and poor patient cooperation during the procedure also play a role in the occurrence of residual astigmatism after surgery.
HOW TO PROCEED
Corneal refractive surgery. Patients with residual astigmatism after ablative or femtosecond laser refractive surgery should be observed for at least 3 months postoperatively to ensure that their refraction has stabilized.
Surface ablation. An enhancement is typically possible after surface ablation.4 The procedure is repeated. To prevent the development of haze, mitomycin C is applied to the stromal bed after the ablation, and a tapering regimen of topical steroids is prescribed.
LASIK. When an eye has residual astigmatism after LASIK, an enhancement in the form of surface ablation or a flap relift followed by ablation of the residual stromal bed may be performed.4
SMILE. A Circle enhancement with the VisuMax femtosecond laser (Carl Zeiss Meditec) may be performed. The SMILE cap is converted into a femtosecond LASIK flap, and the residual stromal bed is treated with excimer laser ablation.5
Cataract surgery. Residual astigmatism can be managed with a corneal or lenticular approach. How best to proceed depends on factors such as the cause and magnitude of astigmatism and the time of presentation.2
Corneal approaches. Surface ablation and LASIK are generally preferred when the amount of residual astigmatism is less than 1.00 D. SMILE is an option for treating between -0.75 and -1.75 D of residual astigmatism.6
Multifocal IOLs decrease patients’ contrast sensitivity. Corneal refractive surgery enhancements should be avoided in this population because they could reduce contrast sensitivity further. Limbal relaxing incisions may be an effective strategy when the amount of residual astigmatism is low and keratorefractive surgery is not an option.
Lenticular approaches. A lens-based enhancement is worth considering when the amount of residual astigmatism is greater than 1.00 D and keratorefractive surgery is contraindicated. IOL repositioning is a reasonable option for addressing lens tilt and toric IOL malrotation.2,7 The ideal timing of both IOL repositioning and exchange is within 12 weeks of the original surgery when the probability of capsular fibrosis and/or phimosis is low. A third lenticular approach is to place a phakic IOL in a piggyback fashion; this can avoid complications related to a fibrosed or unstable capsular bag (Figure).8
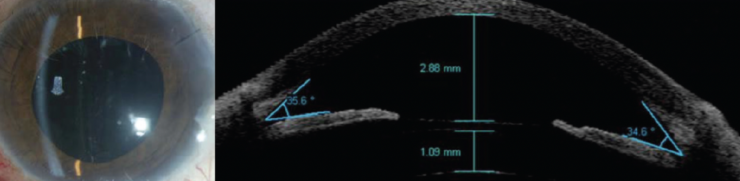
Figure. A Visian ICL (STAAR Surgical) is implanted in a pseudophakic eye with residual high myopic astigmatism after cataract surgery.
CONCLUSION
The ability of AI to predict patients’ subjective refractions before and after refractive surgery is being studied.9,10 The technology has the potential to improve patient selection and the choice of surgical technique, which may ultimately reduce or eliminate the occurrence of residual astigmatism after cataract and refractive surgery.
1. Archer TJ, Reinstein DZ, Piñero DP, Gobbe M, Carp GI. Comparison of the predictability of refractive cylinder correction by laser in situ keratomileusis in eyes with low or high ocular residual astigmatism. J Cataract Refract Surg. 2015;41(7):1383-1392.
2. Moshirfar M, Thomson AC, Thomson RJ, Martheswaran T, McCabe SE. Refractive enhancements for residual refractive error after cataract surgery. Curr Opin Ophthalmol. 2021;32(1):54-61.
3. Han T, Shang J, Zhou X, Xu Y, Ang M, Zhou X. Refractive outcomes comparing small-incision lenticule extraction and femtosecond laser-assisted laser in situ keratomileusis for high myopia. J Cataract Refract Surg. 2020;46(3):419-427.
4. Spadea L, Di Gregorio A. Enhancement outcomes after photorefractive keratectomy and laser in situ keratomileusis using topographically guided excimer laser photoablation. J Cataract Refract Surg. 2005;31(12):2306-2312.
5. Siedlecki J, Luft N, Mayer WJ, et al. CIRCLE enhancement after myopic SMILE. J Refract Surg. 2018;34(5):304-309.
6. Semiz F, Lokaj AS, Musa NH, Semiz CE, Demirsoy ZA, Semiz O. SMILE for the treatment of residual refractive error after cataract surgery. Ophthalmol Ther. 2022;11(4):1539-1550.
7. Sáles CS, Manche EE. Managing residual refractive error after cataract surgery. J Cataract Refract Surg. 2015;41(6):1289-1299.
8. Navas-Pérez A, Ramírez-Miranda A, Gómez-Bastar A, Ramírez-Luquín T, Graue-Hernández E. Implantable collamer lens in pseudophakic high myopia. The Pan-American Journal of Ophthalmology. 2010;9:29-31.
9. Achiron A, Gur Z, Aviv U, et al. Predicting refractive surgery outcome: machine learning approach with big data. J Refract Surg. 2017;33(9):592-597.
10. Rampat R, Debellemanière G, Malet J, Gatinel D. Using artificial intelligence and novel polynomials to predict subjective refraction. Sci Rep. 2020;10(1):8565.
