
CASE PRESENTATION
A 63-year-old man is referred for a refractive surgery evaluation. The patient has mild pigmentary glaucoma in each eye. He underwent bilateral myopic LASIK more than 20 years ago and consecutive (1 week apart) bilateral cataract surgery with implantation of an AcrySof PanOptix trifocal toric IOL (Alcon) about 1 month ago. Figures 1 and 2 show the preoperative biometry and topography measurements, respectively.
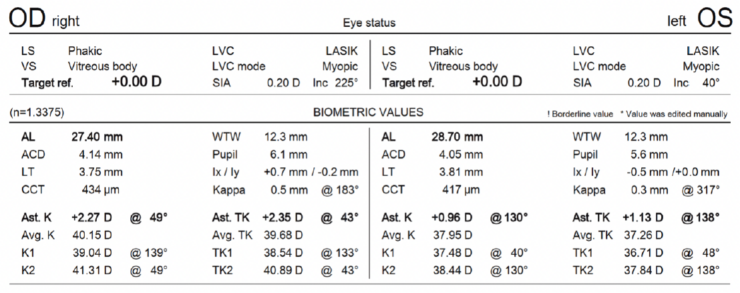
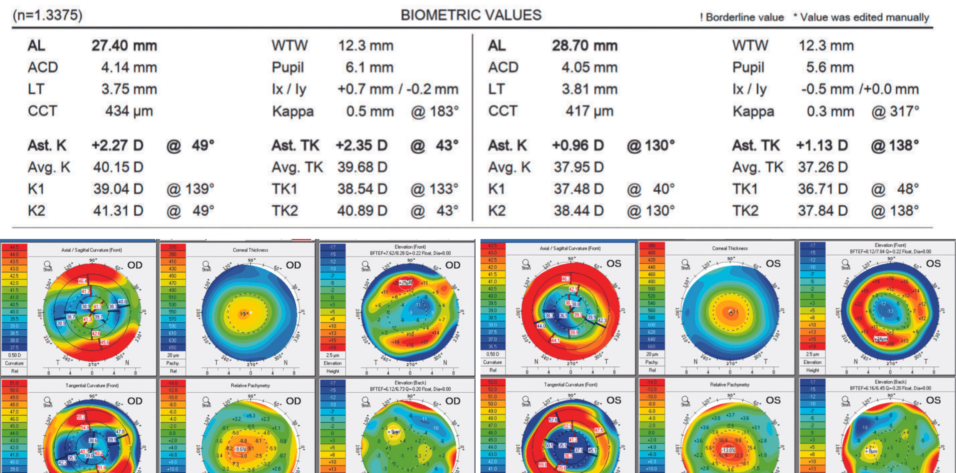
Figure 1. Preoperative biometry measurements.
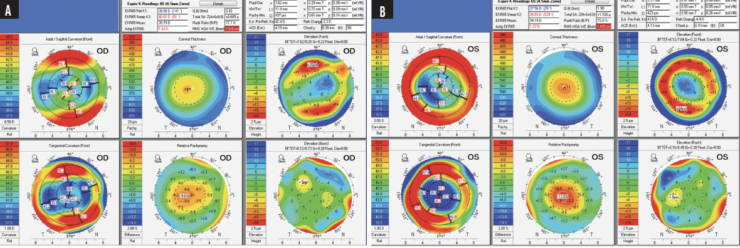
Figure 2. Preoperative topography of the right (A) and left (B) eyes with the Pentacam (Oculus Optikgeräte).
On examination, the patient’s uncorrected distance visual acuity is 20/60 (pinhole acuity 20/40) OD and 20/25+2 OS. His uncorrected near visual acuity is J3 OD and J1 OS. The patient is happy with the vision in his left eye but says the vision in his right eye is waxy and distorted. His manifest refraction is plano OS and -2.25 +1.25 x 82º OD. Quality of vision in the right eye does not improve with refraction.
A slit-lamp examination of both eyes finds well-centered IOLs without tilt. The IOL in the right eye is oriented to the correct axis (45º). Trace punctate staining is evident for both corneas. A fundus examination of each eye is within normal limits, and macular OCT imaging demonstrates normal foveal contour in each eye.
The patient wishes to maintain presbyopic correction in the right eye because he enjoys the visual range in his left eye. How would you proceed?
—Case prepared by Marjan Farid, MD


MIRA AMIN, MD, AND KAROLINNE MAIA ROCHA, MD, PHD
When determining patient candidacy for a multifocal IOL, it is imperative to consider their lifestyle, examine them for ocular surface disease, and assess their optical quality. Figure 1 shows that the patient has high myopia (evidenced by long axial length) and flat (oblate) corneas with residual oblique astigmatism (astigmatism measured by total keratometry was 2.35 D @ 43º). Figure 2 shows a relatively regular bow tie appearance to the astigmatism within the visual axis and high positive spherical aberration in each eye, likely a result of the myopic ablation with a small optical zone. Increased corneal spherical aberration like this can lead to suboptimal postoperative results with multifocal IOLs. Given the irregular astigmatism and greatly increased spherical aberration, it is surprising that the patient’s uncorrected distance visual acuity is 20/25 OS.
Optimization of the ocular surface is essential before surgical intervention. Because his quality of vision does not improve with refraction, an enhancement to correct any residual refractive error is not an option. We would recommend exchanging the IOL for one with negative spherical aberration to offset the positive corneal spherical aberration. An enhanced monofocal toric lens in this category would likely provide him with the best possible quality of vision, but an extended depth of focus toric IOL is an option if the patient prefers.
A formula that takes postrefractive corneal curvature into account, such as the Barrett True-K, would be used for the IOL power calculation. Verifying the magnitude and axis of astigmatism with intraoperative aberrometry might also be helpful.

ABI TENEN, MBBS(HONS), FRANZCO
An AcrySof PanOptix trifocal toric IOL sitting behind a cornea that was previously flattened by LASIK for what looks like a moderate to high myopic refraction is less likely to deliver optimal quality of vision. The patient would be counseled accordingly. If he chose the IOL over alternatives such as a monofocal (with or without monovision) or an extended depth of focus lens, then he would be reminded that he accepted this risk when he consented to surgery.
The patient’s expectations aside, surgery seems to have gone well for both eyes based on the symmetrical result on objective examination. The patient is happy with the vision and plano refraction in his left eye but unhappy with waxy, distorted vision in his right eye, which has a nonsensical refraction. It is possible that subclinical fluid changes are present in the LASIK flap interface in the right eye, particularly because it was cut with a microkeratome and therefore did not heal the same way as a flap created with a femtosecond laser would. If fluid changes are the issue, they should resolve with time. The patient would be reassured that only 1 month has elapsed since cataract surgery. Because his left eye is doing well and both eyes look the same, I would not consider additional surgery at this point and would ask him to return in 3 months. In the meantime, treatment with a suitable lubricant would be initiated to treat the dry corneas.
At 3 months, the patient’s dry eye, visual acuity, and refraction would be reassessed. If a moderate improvement in symptoms is achieved, he may be satisfied, even if the visual acuity in his left eye is still better than in his right. If no improvement is observed, however, then an IOL exchange would be an option but at the expense of multifocality. The procedure, moreover, poses considerable risk, so it would not be my preference. The case presentation makes no note of posterior capsular opacification. It is worth mentioning, however, that it would be prudent to avoid an Nd:YAG capsulotomy in case the patient opts to undergo an IOL exchange in the future.

WHAT I DID: MARJAN FARID, MD
The case underscores the importance of a detailed evaluation of topography and/or tomography in a patient with a history of LASIK who desires a multifocal IOL. The left eye did well with a trifocal IOL, but the quality of vision in the right eye was suboptimal after surgery due to corneal higher-order aberrations (HOAs), as evidenced by an inability to improve his vision with manifest refraction or a rigid gas permeable contact lens overrefraction. Spherical and fourth-order aberrations, moreover, were found on aberrometry with the iTrace (Tracey Technologies). In an eye with significant corneal HOAs like this one, a multifocal optic exacerbates the subtle irregularities and degrades vision.
After 3 months of aggressive ocular surface disease management, manifest refraction failed to improve quality of vision in the patient’s left eye. He and I had a long discussion of his options and their risks and benefits. We decided an IOL exchange would be the most effective way of reducing his optical HOAs. Knowing that the IOL in his left eye would provide a multifocal range and functional near vision, the patient chose an enhanced monofocal toric lens targeted for distance vision for his right eye. An IC-8 Apthera IOL (Bausch + Lomb) would have been another option for this eye with central corneal irregularities secondary to LASIK.
Postoperatively, the patient’s UCVA was 20/25 OD, and his residual refraction was -0.50 +0.50 x 68º OD.