


CASE PRESENTATION
A 62-year-old man was referred to my clinic for complex cataract surgery in his right eye, in which he had suffered a traumatic injury at age 9 years. The patient stated that vision was “never good” in the affected eye after the injury, but he reported progressive worsening during the past several years to the point of “no vision” upon presentation (Figure).
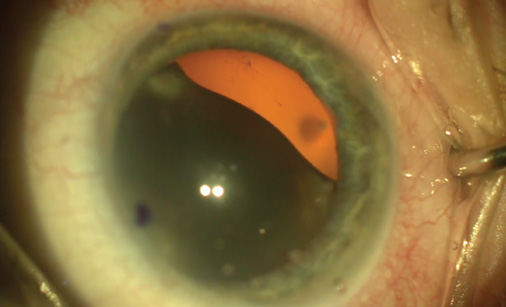
Figure 1. The patient’s right eye had a dense black cataract that was dislocated superotemporally.
On examination, the distance UCVA was count fingers at 1 foot in the patient’s right eye and 20/30+1 in his left. The slit-lamp examination of his right eye was remarkable for a dense black cataract that was dislocated superotemporally. The nasal equator of the cataract was visible, there was a zonular dialysis nasally of at least 5 clock hours, and the nasal margin of the lens had a flattened curvature. Significant iridodonesis and phacodonesis were present. The nasal peripheral retina was visible through the zonular dialysis and was unremarkable. B-scan ultrasound showed no retinal detachment, vitreous opacity, or mass. The patient’s left eye had an early nuclear sclerotic cataract and trace epiretinal membrane.
After discussing with the patient the risks and benefits of cataract extraction with IOL implantation in the right eye, what would your surgical plan be? How would the IOL be supported? Is there a role for a femtosecond laser or other specialized tools?

KENNETH BECKMAN, MD, FACS
This patient has a history of trauma and little lens support. Additionally, he likely has poor visual potential. As with any complicated case, the surgeon should always overprepare. In these situations, regardless of the approach I take, I prefer to have a retina specialist on hand because the lens is at increased risk of dropping into the vitreous. I also prefer to have backup IOLs available in case I need to change my plan on the fly.
Because there are at least 5 clock hours of zonular dehiscence, the remaining zonules may not be very strong. Therefore, I would expect to be unable to place an IOL in the bag. In my experience, unless sewn to the sclera, capsular tension rings do not stay in place long term when the zonular damage is so extensive. If that maneuver is actually required, there are much easier and simpler treatment methods.
First, for the cataract removal itself, I think it would be reasonable to see if the zonular support is adequate to attempt a capsulorrhexis, placement of capsular support hooks, and lens removal with traditional phacoemulsification—but I suspect not. If the lens has completely dislocated, it could be expressed, but that would require a large incision and a prolonged healing time. I would therefore ask the retina specialist to perform a pars plana vitrectomy and remove whatever lens material I could not extract traditionally.
Certainly a femtosecond laser could be used to assist with the capsulotomy and lens fragmentation, but this approach might be difficult because of the lens position and density. Similarly, although the Zepto Capsulotomy System (Mynosys Cellular Devices) and miLoop (IanTech) can be helpful in complex cases, the extra intraocular manipulation might be difficult to perform and too traumatic for this eye.
After the lens has been extracted, there would be multiple possible approaches to the implant. The simplest and perhaps most practical method in this case might be the placement of an anterior chamber IOL. As long as the lens fits well and the angle is normal, I think this approach would be a quick and easy fix.
Surgeons comfortable with scleral fixation of posterior chamber IOLs could pursue this option instead. I would note that, although scleral suturing is familiar to many ophthalmologists, the Yamane technique of externalizing the haptics through the sclera is a quick and elegant procedure.1

KHIUN F. TJIA, MD
I would pursue the simplest solution for this extremely challenging case. I would create a 10-mm sclerocorneal tunnel incision. After injecting diluted triamcinolone and removing any visible vitreous strands, I would inject a dispersive OVD behind and in front of the black cataract.
I would introduce a large loop behind the lens with one hand and a bent needle with my other hand, and then I would trap the lens between the two instruments. Next, I would attempt a manual intracapsular cataract extraction, which would likely be successful given the significant phacodonesis. I would perform repeated injections of triamcinolone, complete a vitrectomy, and then instill a miotic agent.
My preference would be to implant an iris-fixated Artisan IOL (Ophtec). The peripheral iris should be stable enough to ensure sufficient support and stable fixation.

WHAT I DID:
CATHLEEN M. McCABE, MD
I discussed with the patient the risks of cataract surgery complicated by a dense, dislocated cataract in an eye with zonular dialysis. I also explained the uncertain visual benefit, given his long history of poor vision in his right eye. I then recommended cataract extraction and the placement of a scleral-fixated IOL.
My surgical plan included a two-port pars plana vitrectomy with a 23-gauge trocar system. I placed the trocars 3 mm posterior to the limbus, one superonasally for the infusion and one inferotemporally for the vitrector. I filled the anterior chamber with a dispersive OVD (Viscoat, Alcon) through a paracentesis.
The dense cataract was loose, and there was a large zonular dialysis nasally. I created a scleral tunnel incision temporally that had an external length of approximately 5 mm and an internally flared configuration. Next, I performed anterior vitrectomy; I carefully removed vitreous adjacent to the lens and fully mobilized the cataract without dislocating the lens posteriorly. I used a dispersive OVD to protect the endothelium while raising the cataract and capsular bag into the anterior chamber.
After instilling additional OVD in front of and behind the cataract, I opened the scleral incision to its full diameter. I used the miLoop to bisect the lens and capsule so that I could remove the large, dense cataract through a relatively small incision. I introduced the nitinol filament into the anterior chamber and extended it. The loop was carefully passed around the lens and capsule and then was slowly closed, cutting the lens and capsule in half. I used a second instrument through the main incision to free the closed loop from the dense center of the cataract. With a lens loop, I removed the nuclear fragments.
I performed a thorough anterior vitrectomy. With a PTFE suture, I fixated an Akreos AO60 lens (Bausch + Lomb) to the sclera through two sets of sclerotomies placed 2 mm posterior to the limbus and 4 mm apart. I closed the conjunctiva with an 8-0 polyglactin suture and secured the scleral incision with three interrupted 10-0 nylon sutures. I instilled triamcinolone/moxifloxacin compounded solution (Imprimis Pharmaceuticals) in the posterior segment through the trocar and then removed the trocars.
Postoperatively, the patient regained 20/100 distance BCVA in the operated eye. I believe this case represents a novel use of the miLoop for performing a small-incision intracapsular cataract extraction.
1. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
