


Residual refractive errors after cataract surgery have become less common thanks to advances in optical biometry, modern IOL power calculation formulas, and IOL designs. Still, many patients may nonetheless experience a refractive surprise. This can be discouraging to both the patient and physician—in some cases even resulting in loss of a patient or accusations of having performed surgery on the wrong lens.
Even with formulas specifically designed for use after corneal refractive surgery and with the benefit of intraoperative biometry, post-LASIK patients especially are still at an elevated risk for residual refractive error. Fortunately, there are several possibilities to correct postoperative ametropia, including laser vision correction, lens exchange, and implantation of a secondary IOL with a piggyback technique. In appropriate cases, a piggyback IOL could be the best option.
OPTIONS AFTER LASIK
As mentioned, the patients most at risk for postcataract surgery ametropia are those who have previously undergone LASIK. Typically, after myopic LASIK, residual postcataract refractive errors are on the hyperopic side. These are often the patients who most desire spectacle independence; after all, they underwent LASIK in the first place to reduce or eliminate their dependence on glasses.
Although lens exchange is an option in these patients, refractive predictability can be tricky with a new IOL. Furthermore, to get the best idea of residual refractive error and effective lens position, one should delay the exchange at least 1 month after the original surgery. This means the lens will be further scarred into the capsular bag, making the procedure that much more risky.
Because these patients have already undergone laser vision correction, repeat LASIK is typically avoided. Surface ablation is another option, but hyperopic PRK can regress, and it also carries the associated risks of PRK, including postoperative discomfort and exacerbation of dry eye disease—something common in this population.
PIGGYBACK TO THE RESCUE
There are several reasons why piggyback IOL may be the best option for patients who have had myopic LASIK. These patients tend to have longer than average eyes, and their sulcus space is generally large enough to support a piggyback IOL. Additionally, the refractive predictability of piggyback IOLs is highly reliable. Although refractive vergence formulas can be employed, for smaller errors one can simply multiply the hyperopic refractive error by 1.5 to determine the proper piggyback IOL power; for myopic errors, the formula is modified so that the error is multiplied by 1.3. (Note: Some surgeons prefer to multiply by 1.2).
The surgery itself is often quick and straightforward. I make a 2.75-mm incision and inject an LI61AO SofPort lens (Bausch + Lomb) into the sulcus (Figure). This IOL has several attributes that make it ideal in this scenario. First, it is made of silicone, so there is no concern for interlenticular opacification. Second, it injects in a planar fashion, making placement in the sulcus easy. Third, if a patient with an in-the-bag acrylic IOL has complaints of negative dysphotopsias, this lens can reduce those unwanted optical phenomena.
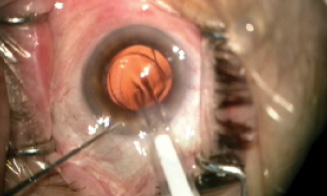
Figure. The piggyback lens is implanted in the eye.
Surgical recovery is rapid. Inflammation from the procedure is minimal, and patients appreciate the improvement almost immediately. Piggyback IOLs have shown excellent long-term stability, and in appropriate situations they can be an outstanding option for treatment of postcataract ametropia.
CONCLUSION
Today we have a variety of options to correct our patients’ refractive errors, and these options—laser vision correction, lens exchange, and piggyback IOL—extend to postoperative residual refractive errors. In appropriate cases including post-LASIK patients, a piggyback IOL could be the best option.

