





Debate over IOL nomenclature* has become the topic of conversation internationally.1 The volume of presbyopia-correcting IOLs available worldwide is increasing, and lenses are now being labeled with terms that confuse rather than clarify matters.
THE BASICS
A review of the basics may shed some light on the best use of IOL terminology in modern anterior segment surgery.
Lens design. Multifocality has one of two specific designs, refractive and diffractive. IOLs with a refractive design are made with different zones or asphericities of the lens that are manipulated to achieve multifocality. IOLs with a diffractive design have sawtooth-like diffractive rings on a monofocal base. Both types of lenses provide a range of vision that may include distance and intermediate with or without near vision. It is important to note that reading distances vary with the object of focus and among individuals.
Lens function. A common misconception is that the lens itself influences patient outcomes. The lens is an important variable, but the cornea and its inherent aberrations as well as pupil size and axial length influence outcomes. The modulation transfer function (ie, optical performance of the optical system) is based on the combined influences of the tear film, cornea, IOL, vitreous, and pupil size. A small pupil will greatly enhance range of visual performance independent of the lens type.
Postoperative side effects. No lens currently exists that provides full spectacle independence and no photic phenomena. We are still learning about how dysphotopsias such as halos, glare, and starbursts may affect postoperative vision. The presence of dysphotopsias typically improves with neural adaptation. When patients are counseled well preoperatively, satisfaction can be high, and there is typically a low requirement for explantation.
Reduced contrast sensitivity with multifocal IOLs may be problematic; however, this challenge is possibly more theoretical than real. As a fixed amount of light enters the eye, the light is split and shared between the different foci of the lens.
MAKE IT EASY FOR THE PATIENT
In the past 4 years, terms such as extended depth of focus (EDOF), extended range of vision, and nondiffractive have emerged to classify certain types of IOLs. These terms, however, often confuse patients and ophthalmologists. A simpler naming convention system has been proposed (see the article “Let’s Speak Lenspeak,” also published in this issue).
The problem is that lens functionality, mechanism of action, and magnitude and type of photopsias are discussed interchangeably and are therefore confusing. If the term EDOF remains in use in the market, it should be reserved for aperture-based IOLs. Current EDOF IOLs are best categorized by functionality (eg, increased range or depth of focus and full range of focus), but the criteria might need revision. The mechanism of action and in turn presence, type, and magnitude of photopsias would relate to the lens mechanism of action and be based on real-world evidence.
Most patients do not care about the terminology and optic principles (ie, diffractive, refractive); they care about the expected endpoints of spectacle independence, range of unaided vision, and quality of vision.
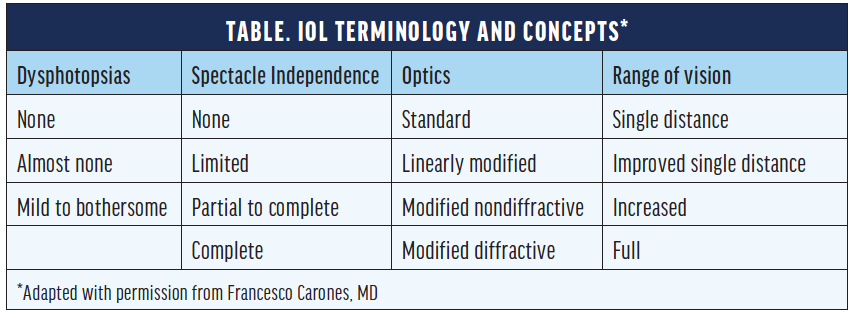
Francesco Carones, MD, from Carones Vision in Milan, Italy, uses the mantra listen, measure, share as a reminder of how to satisfy patients’ expectations. Listen to what the patient wants, take appropriate preoperative measurements, and share the recommended lens types with the patient. He describes these lenses to patients not with the terms we typically hear as practitioners but by the lenses’ benefits to patients. He discusses four concepts with them, which are spectacle independence, range of vision (distances), dysphotopsia, and optics (Table). Defining IOLs by the level of spectacle independence they provide and their optics (mechanism of action) can help surgeons and patients make educated decisions together about suitable lens choices.
REACH A CONSENSUS
For both younger and older ophthalmologists and, in particular, for patients, the misguided use of IOL terminology is confusing. A consensus must be reached as a community of ophthalmologists and manufacturers categorizing IOLs. Let’s work to intensify this discussion and eventually produce a classification system accepted by the ophthalmic community as a whole.
*This article reviews some of the points discussed during a Refractive Surgery Alliance Journal Club meeting.
1. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020. Ophthalmology. September 25, 2020. doi:10.1016/j.ophtha.2020.09.026
