



Cataract surgery has become a refractive procedure in the developed world. IOL power calculations, however, remain challenging because the effective lens position (ELP), or exact postoperative physical position of the IOL, must be derived from a host of preoperative data points and proprietary formulas. The optical outcome of surgery also depends on proper centration and fixation of the IOL. For aspheric IOLs to be effective, they must be accurately centered, and significant tilt must be avoided.1,2 This is true not only in the early postoperative period but also over the long term. Multifocal IOLs with diffractive optics and extended depth of focus IOLs are particularly sensitive to tilt and decentration. Variance in the optical center from the center of the visual axis with extended depth of focus IOLs can also induce higher-order optical aberrations, increase dysphotopsia and other visual side effects, and reduce subjective quality of vision. The astigmatic correction offered by toric IOLs decreases with every degree of postoperative rotation.
Currently Available Anterior Capsulotomy–Fixated IOLs With the CE Mark
At present, three IOLs with the CE Mark are manufactured specifically for anterior capsulotomy fixation:
- Tassignon Bag-in-the-Lens (Morcher): This haptic-free IOL is designed such that the anterior and posterior capsulotomies are captured in an equatorial groove (Figure 1).
- Femtis (Oculentis): This plate haptic lens features four struts or tabs that fixate the optic to the anterior capsulotomy (Figure 2).
- Masket 90S IOL (Morcher): This IOL features a groove in the optic edge that captures the anterior capsulotomy, fixating the optic (Figure 3).
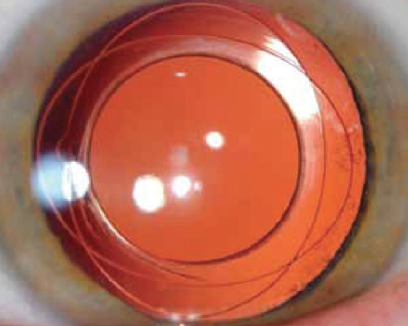
Figure 1. The Tassignon Bag-in-the-Lens has two opposing ovals with an equatorial groove that accepts both anterior and posterior capsulotomies.
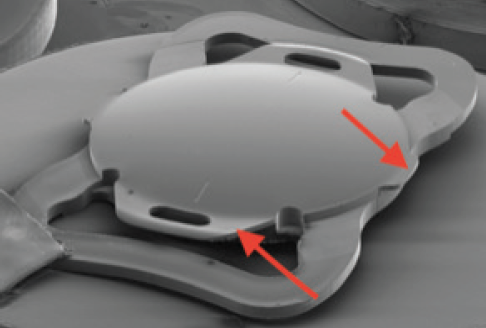
Figure 2. The Femtis IOL has four struts (arrows indicate two of the four) on the anterior optic that capture the anterior capsulotomy.
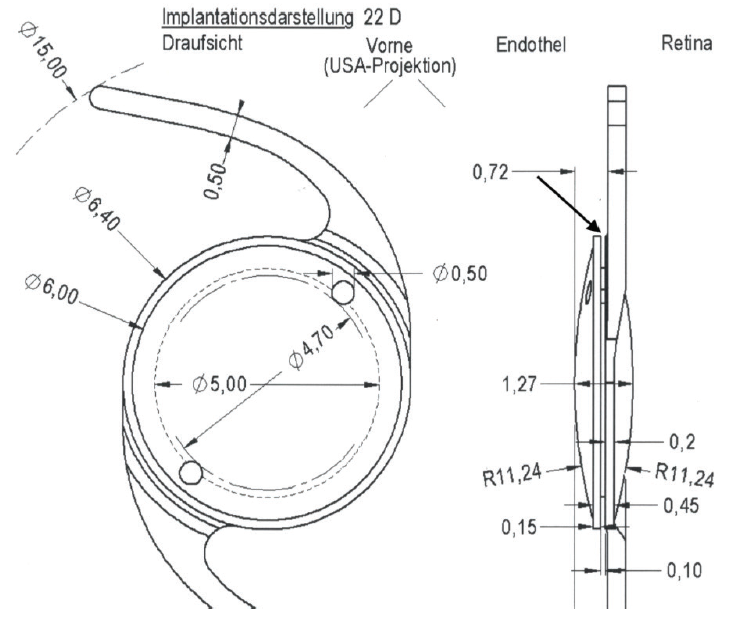
Figure 3. Schematic of the Masket 90S IOL. Note the fixation holes and groove (oblique arrow upper right) that accepts the anterior capsulotomy.
Given the difficulty of predetermining the ELP, those attempting to address it are likely to be left wondering, “How can we achieve these seemingly lofty goals?”
The Current Standard and Its Challenges
The state of the art in cataract surgery is to place the IOL within the empty capsular bag remnant after performing a continuous circular anterior capsulotomy and phacoemulsification. The capsulotomy is typically designed to overlap the anterior edge of the optic symmetrically for approximately 0.50 mm. Postoperatively, fibrous metaplasia of the residual lens epithelial cells can cause the capsular bag to shrink wrap around the haptics and optic of the IOL. Asymmetric fibrosis and other factors may cause the IOL to rotate, become decentered, or tilt inside the capsular bag.3,4 Some surgeons aggressively curette or aspirate the residual anterior subcapsular lens epithelial cells, whereas others leave the cells undisturbed. Varying with the degree to which the capsular remnant shrinks, the change in IOL position may induce ametropia and higher-order optical aberrations that may progress over time. Optical outcomes may therefore be different at 6 weeks and 6 months.
Additionally, although most IOLs are uniform in size, the capsular bag is not, which may result in decentration or rotation of the IOL during or immediately after surgery. Postoperative rotation of a toric IOL is more likely in a myopic eye with a large capsular bag.5
Anterior Capsulotomy IOL Fixation: A Better Option?
The key factors in achieving and maintaining ideal optical outcomes after cataract surgery are short- and long-term alignment of the optical axis of the IOL with the visual axis of the eye, long-term stability of the spherical outcome of surgery, prevention of toric IOL rotation, and a better estimation of the ELP. Anterior capsulotomy fixation of the IOL can help to achieve these goals. The sidebar on the previous page provides a brief overview of the three anterior capsulotomy-fixated IOLs with the CE Mark.
With preoperative image-guidance tools that are registered with a femtosecond laser (or another automated device), the anterior capsulotomy can be sized appropriately and centered on the visual axis. In turn, the grooved IOL, when captured in the capsulotomy, should also be perfectly centered on the visual axis, optimizing visual outcomes with all types of premium IOLs and eliminating issues associated with angle kappa or chord mu and other causes of IOL decentration. Additionally, because the optic is choked by the capsulotomy, it will not move inside the bag after surgery, and capsular phimosis cannot occur, likely preserving stable optical outcomes over the long term. In a 2020 report regarding the Femtis IOL (Oculentis), the median shift in IOL position from surgery to 6 months postoperatively was 0.09 mm.6 With capsulotomy capture of the optic, off-axis rotation of a toric IOL cannot occur after surgery.6
Additional Benefits
ELP could be more predictable, given that the optic is not likely to shift postoperatively. Lukan Mishev, MD, investigated this concept in a small trial in Bulgaria. He demonstrated that the anterior chamber depth in one eye that received the Masket 90S IOL (Morcher) did not vary more than 0.01 mm over a 30-day period (Figure). In contrast, in another eye with a standard in-the-bag IOL, there was a sevenfold greater fluctuation during the same period (unpublished data, Mishev, March 2018). I look forward to further studies of this facet of capsulotomy fixation of the IOL.
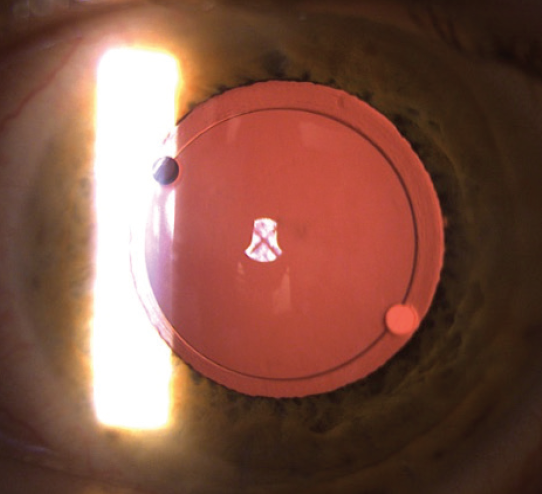
Figure. A Masket 90S IOL in the left eye 1 day after surgery. Note centration on the visual axis.
Courtesy of Tobias H. Neuhann, MD, FEBOS-CR
Another advantage of anterior capsular fixation of the optic is the elimination of negative dysphotopsia, which is the concept that motivated the design of the Masket 90S IOL.7 Negative dysphotopsia has not been reported with any capsulotomy-fixated IOL.6,8
conclusion
Capsulotomy fixation and automated centration of the capsulotomy on the visual axis permit alignment of the optic and visual axes, which results in a higher-quality, more stable visual outcome than previously possible.
1. Athena Z, Maqsood S, Ahmed SN, Nanavaty MA. Effect of intraocular lens tilt and decentration on visual acuity, dysphotopsia and wavefront aberrations. Vision (Basel). 2020;4(3):41.
2. Liu X, Xie L, Huang Y. Effects of decentration and tilt at different orientations on the optical performance of a rotationally asymmetric multifocal intraocular lens. J Cataract Refract Surg. 2019;45(4):507-514.
3. Hayashi K, Hayashi H, Nakao F, Hayashi F. Anterior capsule contraction and intraocular lens decentration and tilt after hydrogel lens implantation. Br J Ophthalmol. 2001;85(11):1294-1297.
4. Findl O, Hirnschall N, Draschl P, Wiesinger J. Effect of manual capsulorhexis size and position on intraocular lens tilt, centration, and axial position. J Cataract Refract Surg. 2017;43:902-908.
5. Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38(1):54-59.
6. Darian-Smith E, Versace P. Visual performance and positional stability of a capsulorhexis-fixated extended depth-of-focus intraocular lens. J Cataract Refract Surg. 2020;46(2):179-187.
7. Masket S. Development of an anti-dysphotopic IOL. 2019. Expert Rev Ophthalmol. doi:10.1080/17469899.2018.1560263
8. Masket S, Fram NR, Cho A, Park I, Pham D. Surgical management of negative dysphotopsia. J Cataract Refract Surg. 2018;44(1):6-16.
