



It is difficult to achieve the desired results after refractive surgery for hyperopia, even with modern technology. The greatest obstacle is arguably postoperative regression, which is typically more significant after hyperopic than myopic treatment.
CAUSES OF REGRESSION
Postoperative regression is a multifactorial process involving the corneal epithelium, inflammatory cascades, limbal stem cells, and the corneal stroma. After hyperopic treatment, the regression is most likely caused by the epithelial response to the corneal ablation and to stromal biomechanics. In short, the laser ablation causes cytokine-mediated wound-healing cascades that replenish stromal tissue removed during the refractive procedure.
Further, the prolonged elevation of cytokine signaling and keratocyte apoptosis in areas abutting where corneal tissue was removed may lead to corneal thinning and changes in shape that alter the eye’s refractive status.
The use of corneal allograft inlays is being explored as a way to avoid these responses and achieve more predictable outcomes.
A PROMISING IDEA
Investigations of lenticule implantation in the cornea date back to Barraquer’s work in 1949.1 Inadequate tissue preparation at that time, however, led to unpredictable results, and interest in the method remained low until the advent of SMILE. A recent avenue of research is the implantation of the lenticule extracted during myopic SMILE into a hyperopic eye.2
Allograft lenticule implantation offers many advantages for refractive correction. Perhaps the most important of these is the procedure’s reversibility, meaning the lenticule can be removed if desired. Moreover, unlike hyperopic excimer laser ablation, lenticule implantation does not involve laser ablation or the removal of tissue, so the procedure should not induce the same level of compensatory corneal stromal response and wound-healing cascades.
REVIEWING THE EARLY RESULTS
Study design. At our clinic, we implanted hyperopic allograft corneal inlays (TransForm, Allotex) in 28 eyes of 16 patients with hyperopia. On average, patients were 36.2 ±12.4 years of age. The manifest refraction ranged from 1.00 to 6.00 D, and the cylindrical refraction was less than 1.00 D. A 110-µm corneal flap was created with a femtosecond laser, and a lenticule was implanted underneath and centered on the pupil (Figure 1).
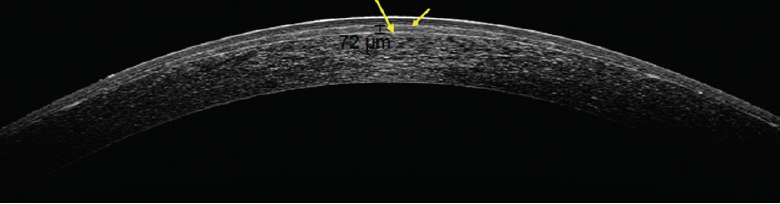
Figure 1. Anterior segment OCT scan of an eye after the implantation of an allograft corneal inlay.
Visual acuity results. At 12 months, the manifest refraction spherical equivalent had decreased significantly. Uncorrected distance and near visual acuities and corrected near visual acuity all had increased significantly. Corrected distance visual acuity remained unchanged.
Regression results. The amount of regression observed during the postoperative period was acceptable. At the end of 12 months, a minimal undercorrection was found (Figures 2–4).
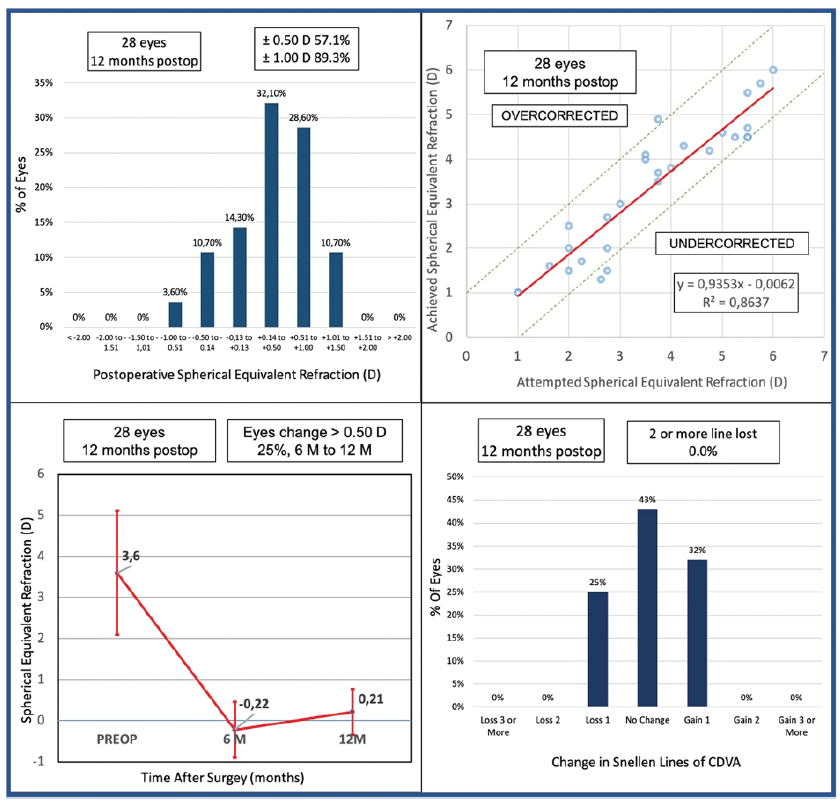
Figure 2. The results of the authors’ study.
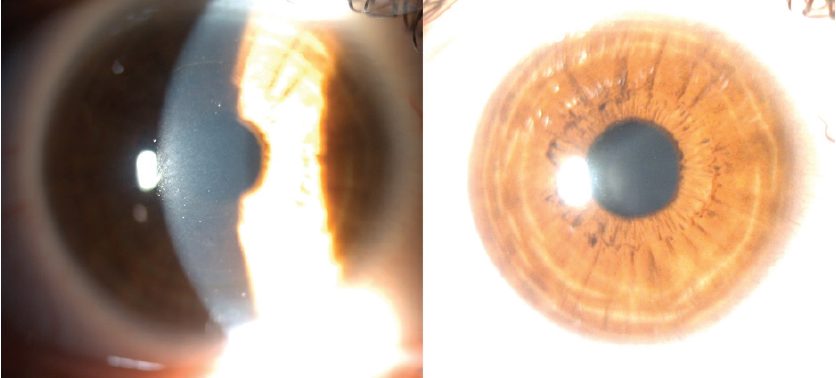
Figure 3. View of an eye 12 months after the implantation of a hyperopic allograft corneal inlay.
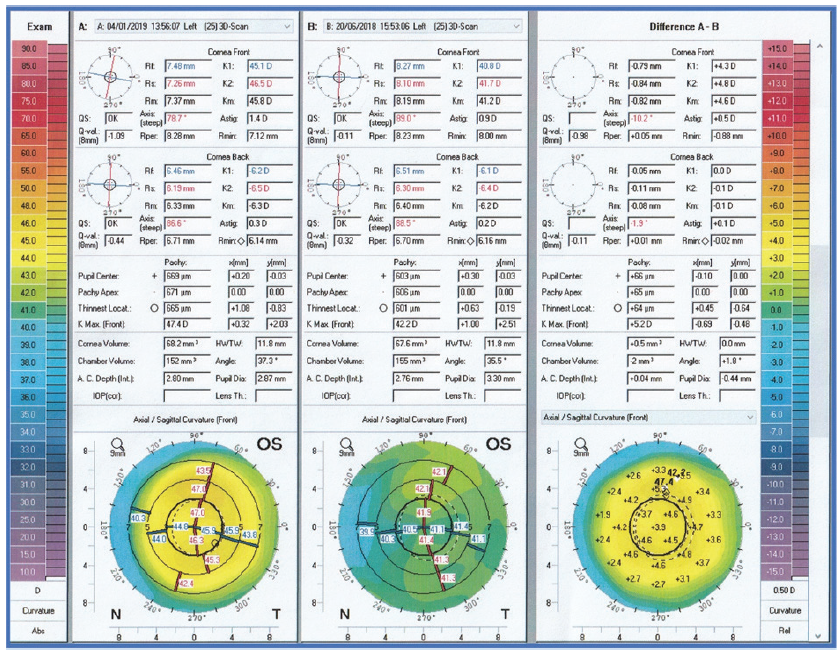
Figure 4. Change in corneal topography after the correction of 4.00 D hyperopia in one eye implanted with an allograft corneal inlay.
Postoperative complications. No serious postoperative complications were observed. Eight patients experienced dry eye symptoms that resolved by 6 months postoperatively. No patient required lenticule extraction.
Serious problems with synthetic corneal inlays have been reported,3 including inlay decentralization, peri-inlay deposits, and a loss of more than 2 lines of vision. We did not, however, encounter any of these with the allogenic implant.
CONCLUSION
Our early experience suggests that the implantation of allogenic corneal tissue is a promising option for the treatment of hyperopia. More work is required to confirm these results.
1. Barraquer JI. Modification of refraction by means of intracorneal inclusions. Int Ophthalmol Clin. 1966;6(1):53-78.
2. Sun L, Yao P, Li M, Shen Y, Zhao J, Zhou X. The safety and predictability of ımplanting autologous lenticule obtained by SMILE for hyperopia. J Refract Surg. 2015;31(6):374-379.
3. Mulet ME, Alio JL, Knorz MC. Hydrogel intracorneal inlays for the correction of hyperopia: outcomes and complications after 5 years of follow-up. Ophthalmology. 2009;116(8):1455-1460, 1460.e1.
