

SMILE has continued to evolve over the past decade. It is now a well-established corneal refractive procedure, as evidenced by the numbers: More than 3.5 million SMILE procedures have been performed globally and more than 2,000 surgeons are offering it in 70 countries. SMILE has become the dominant laser vision correction procedure in Korea and may soon become the dominant procedure in China. Further, SMILE has been studied extensively, with more than 600 published peer-reviewed articles.
In the United States, the volume of SMILE procedures increased significantly this past year despite a negative trend in laser vision correction. This article discusses the current status of SMILE and what to expect in the future.
POTENTIAL ADVANTAGES
The top six current advantages of the SMILE procedure are outlined herein.
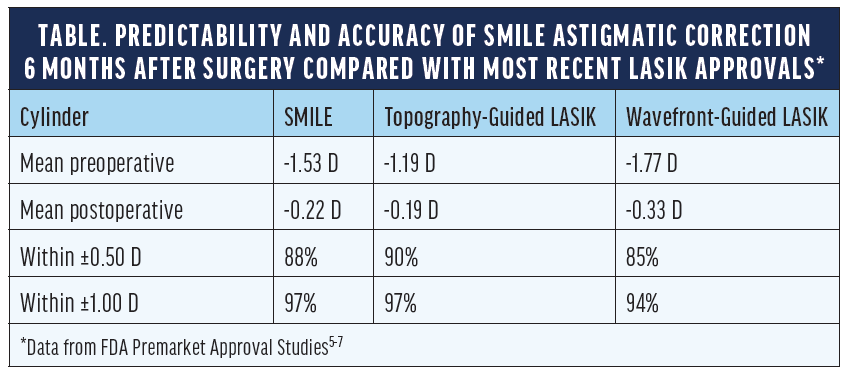
No. 1: Like other laser vision correction procedures, SMILE offers excellent safety, efficacy, and long-term stability. The procedure also often improves low-contrast vision.1-3 A 2019 review of clinical outcomes from premarket approval FDA studies found that SMILE, wavefront-guided LASIK, and topography-guided LASIK all were predictable and safe and produced similar postoperative outcomes.4 Astigmatic corrections as produced by these three procedure types also had similar outcomes in premarket approval FDA studies (Table).5-7
No. 2: As a single-laser procedure that does not require a flap, SMILE avoids intra- and postoperative flap-related concerns. Additionally, many patients are attracted to the small-incision procedure in an era when medical professionals in general are migrating to small-incision surgical technology. It is also possible that SMILE better maintains corneal biomechanical strength compared with LASIK.8
No. 3: There is less impact on perioperative dry eye metrics. Less dry eye in the postoperative period and a faster return of corneal sensitivity have been reported with SMILE compared with LASIK (Figure).9 According to Liu et al, although refractive surgery can affect corneal nerve status long-term, the preservation and regeneration of the corneal nerves were better in eyes that underwent SMILE versus LASIK.10
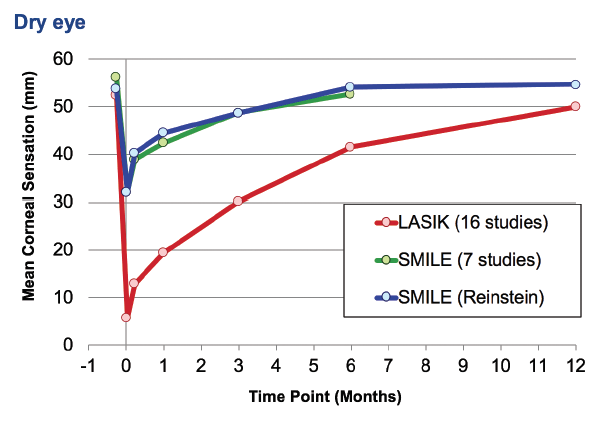
Figure. Mean corneal sensation after LASIK and SMILE.
Courtesy of Dan Z. Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO
No. 4: Updated FDA approvals for SMILE in 2018 expanded treatment indications, allowing the correction of up to -10.00 D of myopia and up to 3.00 D of astigmatism. These approvals also permit the use of a smaller incision (from 90º to 60º) and an adjustment of spot, track, and energy settings. Lower energy settings have improved early visual recovery.11,12 Proper energy levels are important when shaping the lenticule with posterior and anterior incisions.
No. 5: Patients treated with SMILE have reported positive outcomes. A user survey of nearly 500 participants in 50 countries, conducted by Carl Zeiss Meditec in 2020, showed that 56% of participants experienced the same early visual recovery as reported after LASIK, whereas 18% reported that they had even faster visual recovery. When asked how happy they were with their procedure, 97% of participants stated that they were satisfied.
No. 6: SMILE can offer much faster visual recovery than PRK without flap-related concerns. PRK is the refractive procedure most commonly performed on active-duty service personnel in US Department of Defense refractive surgery centers. This is partly due to concerns about the stability of the postoperative LASIK flap to trauma. Many of these centers have now begun offering SMILE. Sia et al performed a retrospective study of the records of service members who underwent myopic SMILE, LASIK, and PRK in the US Department of Defense.13 These investigators reported that, 1 month after surgery, uncorrected distance visual acuity was 20/20 or better in 87.9% of eyes treated with SMILE and 73.8% of eyes treated with PRK. Six months after surgery, 96.3% of SMILE-treated eyes and 83.8% of LASIK-treated eyes had a manifest refraction spherical equivalent within ±0.50 D of target.
CURRENT LIMITATIONS
There are four current limitations of the SMILE procedure.
No. 1: The currently approved laser (VisuMax, Carl Zeiss Meditec) does not provide automated centration. Therefore, proper centration depends on the positioning of the suction ring. This limitation is mitigated by a combination of surgical training and application support, excellent optics, surgical visibility, and curved applanation—the last of which results in less overall suction and greater patient comfort and enables the patient to maintain fixation throughout the procedure. Reduced levels of suction, while beneficial in many ways, have been associated with rare suction loss if there is significant patient movement. This risk decreases as surgeons gain experience with SMILE and through the counseling and guiding of patients before and during the procedure.14
No. 2: The laser does not provide automated cyclotorsional alignment.15 The predictability, however, of astigmatic correction with SMILE is similar to that of the latest LASIK procedures that use automatic cyclotorsional alignment (Table).
No. 3: SMILE is not yet approved for the treatment of hyperopia in the United States or Europe. Researchers, however, are studying this indication. Evaluating eyes treated with vertex-centered hyperopic SMILE, Pradhan et al stated that uncorrected distance visual acuity was 20/40 or better in 95% of eyes (n = 37) with a plano target.16 On a larger scale, researchers recently performed a pivotal international study of hyperopic LASIK; initial results are promising, but data are still being collected and analyzed. Future commercialization is in the planning phase.
No. 4: SMILE cannot correct higher-order aberrations. The procedure is based on the manifest refraction—the aberration that most refractive surgery patients seek to improve. In terms of induced spherical aberration, however, SMILE compares favorably with the latest treatments.17
FUTURE DIRECTIONS
Two future directions of the SMILE procedure are promising.
No. 1: Lenticule transplantation. Investigators around the world are studying potential applications of lenticule transplantation to treat hyperopia and astigmatism as well as its therapeutic indications. Li et al transplanted lenticules from SMILE donors to eight eyes with post-LASIK ectasia, and recipients’ keratocytes appeared to repopulate the lenticules.18 This finding suggests that keratocytes may recover gradually, with the regrowth of subbasal nerves, but additional research is needed.
No. 2: Technological advances. Research has shown that SMILE can help patients achieve optimal visual outcomes to reduce their dependence on glasses. A new generation of the VisuMax laser is being developed, which should increase the speed of the procedure and improve docking, centration, and cyclotorsion compensation.
1. Blum M, Lauer AS, Kunert KS, Sekundo W. 10-year results of small incision lenticule extraction. J Refract Surg. 2019;35(10):618-623.
2. Yan H, Gong LY, Huang W, Peng YL. Clinical outcomes of small incision lenticule extraction versus femtosecond laser–assisted LASIK for myopia: a meta-analysis. Int J Ophthalmol. 2017;10(9):1436-1445.
3. Breyer DRH, Beckers L, Hagen P, et al. Vergleich der langzeitergebnisse bei small incision refractive lenticule extraction (ReLEx SMILE) und femto-lasik. Klin Monbl Augenheilkd. 2019;236(10):1201-1207.
4. Schallhorn JM, Seifert S, Schallhorn SC. SMILE, topography-guided LASIK, and wavefront-guided LASIK: review of clinical outcomes in premarket approval FDA studies. J Refract Surg. 2019;35(11):690-698.
5. US Food & Drug Administration. Premarket Approval Study: VisuMax femtosecond laser lenticule removal procedure for the correction of myopia with or without astigmatism. Accessed January 6, 2021. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P150040S003
6. US Food & Drug Administration. Premarket Approval Study: Allegretto Wave Eye-q excimer laser system. Accessed January 6, 2021. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMA/pma.cfm?id=P020050S012
7. US Food & Drug Administration. Premarket Approval Study: STAR S4 IR excimer laser system with IDesign Wavescan Studio System. Accessed January 6, 2021. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P930016S044
8. Guo H, Hosseini-Moghaddam SM, Hodge W. Corneal biomechanical properties after SMILE versus FLEX, LASIK, LASEK, or PRK: a systematic review and meta-analysis. BMC Ophthalmol. 2019;19(1):167.
9. Cai WT, Liu QY, Ren CD, et al. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a meta-analysis. Int J Ophthalmol. 2017;10(4):632-638.
10. Liu YC, Jung ASJ, Chin JY, Yang LWY, Mehta JS. Cross-sectional study on corneal denervation in contralateral eyes following SMILE versus LASIK. J Refract Surg. 2020;36(10):653-660.
11. Donate D, Thaëron R. SMILE with low energy levels: assessment of early visual and optical quality recovery. J Refract Surg. 2019;35(5):285-293.
12. Li L, Schallhorn JM, Ma J, Cui T, Wang Y. Energy setting and visual outcomes in SMILE: a retrospective cohort study. J Refract Surg. 2018;34(1):11-16.
13. Sia RK, Ryan DS, Beydoun H, et al. Visual outcomes after SMILE from the first-year experience at a U.S. military refractive surgery center and comparison with PRK and LASIK outcomes. J Cataract Refract Surg. 2020;46(7):995-1002.
14. Huang TZ, Shen L, Yu XN, Jin HY. Risk factors and incidence of suction loss during small incision lenticule extraction (SMILE) in 8493 eyes. BMC Ophthalmol. 2020;20(1):412.
15. Chen P, Ye Y, Yu N, et al. Comparison of small incision lenticule extraction surgery with and without cyclotorsion error correction for patients with astigmatism. Cornea. 2019;38(6):723-729.
16. Pradhan KR, Reinstein DZ, Carp GI, Archer TJ, Dhungana P. Small incision lenticule extraction (SMILE) for hyperopia: 12-month refractive and visual outcomes. J Refract Surg. 2019;35(7):442-450.
17. Damgaard IB, Ang M, Mahmoud AM, Farook M, Roberts CJ, Mehta JS. Functional optical zone and centration following SMILE and LASIK: a prospective, randomized, contralateral eye study. J Refract Surg. 2019;35(4):230-237.
18. Li M, Wei R, Yang W, et al. Femtosecond laser-assisted allogenic lenticule implantation for corneal ectasia after LASIK: a 3-year in vivo confocal microscopic investigation. J Refract Surg. 2020;36(11):714-722.